Collision with terrain
Apex Helicopters Inc.
Robinson R44, C-GZFX
Foleyet, Ontario, 17 nm S
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content.
Summary
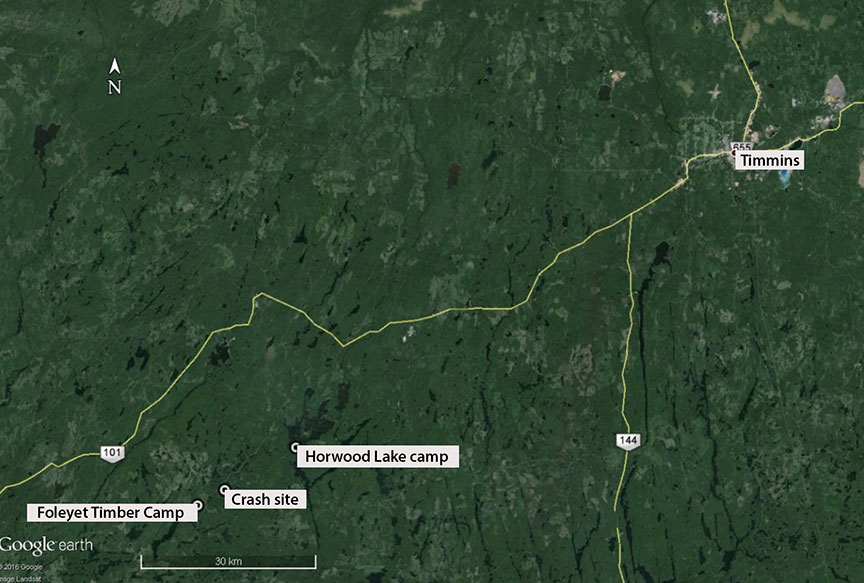
On 08 September 2015, at approximately 2015 Eastern Daylight Time, an Apex Helicopters Inc. Robinson R44 (registration C GZFX, serial number 0595) departed from a camp on Horwood Lake, Ontario, for the Foleyet Timber Camp, 17 nautical miles south of Foleyet, Ontario, with 1 pilot and 1 passenger on board. Approximately 3.1 nautical miles northwest of the Foleyet Timber Camp, the helicopter struck trees on elevated terrain. The occupants sustained fatal injuries. The helicopter was destroyed by impact forces. There was no post-impact fire. The helicopter was equipped with an emergency locator transmitter, but no signal was transmitted or detected by search and rescue agencies. The aircraft was not reported missing until the following day at approximately 1500, at which point search and rescue operations were initiated. The wreckage was discovered by a company aircraft on 11 September.
Le présent rapport est également disponible en français.
Factual information
History of the flight
C-GZFX, operated by Apex Helicopters Inc. (Apex), was on its last day of work on a 4-month forestry tendingFootnote 1 contract for the EACOM Timber Corporation (EACOM). On the morning of 08 September 2015, the pilot travelled by truck from the Foleyet Timber Camp (FTC) to a nearby forestry blockFootnote 2 where the helicopter had been left overnight. On arrival at the forestry block (Figure 1), the pilot performed the normal pre-flight duties. There was a delay in starting the remaining spraying because there was an excessive amount of dew on the trees. At approximately 1030,Footnote 3 the pilot was airborne and made a series of flights to perform the spraying operations required to complete the contract. After the spraying was completed, the aircraft returned to the FTC around 1220. All of the spraying flights were uneventful.
Shortly after the pilot returned to the FTC at the end of his work, the EACOM supervisor arrived at the camp to pick up the end-of-contract paperwork.Footnote 4 The pilot told him that it would be ready in approximately 30 minutes. Shortly afterward, the pilot told the supervisor that he would need more time than originally estimated to complete the paperwork and that he would drive it to the supervisor's camp on Horwood Lake later in the day. The supervisor left the FTC for his camp at approximately 1330.
At approximately 1730, 2 Apex support personnelFootnote 5 left the FTC for Timmins, Ontario, leaving the pilot and one of the mix rig operators at the camp with no vehicle. Once in cell phone range, the 2 support personnel called Apex flight operations to inform them that they were travelling to Timmins to have a piece of equipment repaired. At approximately 1840, the support personnel received a text message from the pilot, asking about the status of the truck repairs and when they would be back. They told him that they would be back around 2100. This was the last communication between the pilot and other Apex personnel.
At approximately 1850, the EACOM supervisor heard a helicopter flying over his camp on Horwood Lake. He then drove to a nearby gravel pit and met the pilot and the mix rig operator, who were on board C-GZFX. They then went to the supervisor's camp, where they reviewed the end-of-contract paperwork and discussed the work that had been performed for the summer contract.
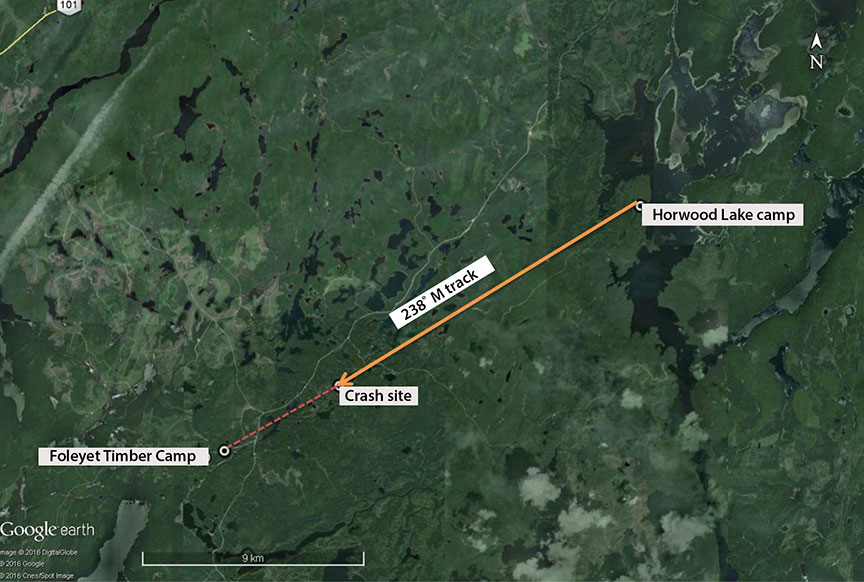
At approximately 2000, the supervisor drove the pilot of C-GZFX and the mix rig operator back to the helicopter and watched them lift off at approximately 2015. Sometime later, C-GZFX struck trees and the terrain at the top of a small hill approximately 8 nautical miles (nm) southwest of the Horwood Lake camp and along the direct route back to the FTC (Figure 2).
At approximately 2130, the 2 support personnel who had gone to Timmins arrived at the FTC and noted that C-GZFX was not there. They found a flight itinerary that indicated that the pilot and the mix rig operator had gone to the EACOM supervisor's camp and would “be back soon.” Because it was dark and the weather was poor, they assumed that the pilot and the mix rig operator had remained overnight at the Horwood Lake camp. No attempt was made to contact the EACOM supervisor or Apex personnel to inform them that the helicopter was overdue.
The planned flight itinerary for the following day was to depart the FTC early in the morning and ferry the helicopter south to the company's main base in Wingham, Ontario. Apex flight operations were not aware that C-GZFX was missing until approximately 1500 on 09 September when the helicopter did not arrive at Wingham. At that time, Apex informed the Joint Rescue Coordination Centre (JRCC) in Trenton and the Ontario Provincial Police South Porcupine detachment that the helicopter was missing, and search and rescue operations began. The wreckage was discovered at approximately 1600 on 11 September by an Apex company helicopter.
Pilot
The pilot held a Canadian Commercial Pilot Licence - Helicopter and had a valid Category 1 medical certificate. The pilot was certified and qualified for the flight in accordance with existing regulations. His medical certificate had a restriction requiring him to wear corrective lenses while flying.Footnote 6 He was not endorsed for night flying, nor did he hold an instrument rating. The pilot had accumulated approximately 268 hours total flight time in helicopters, of which 110 hours were on the Robinson R44 type. He was known to be meticulous at performing his flight and associated administrative duties.
A review of the pilot's work and rest history indicated that he was not likely to have been fatigued at the time of the accident. Trace amounts of alcohol were found in the pilot's system, but these would not have affected his performance. The investigation concluded that there were no physiological factors that would have impeded the pilot's performance of his flight duties.
Weather
The nearest recorded weather for the Foleyet area is taken at Timmins, 40 nm northeast of the FTC. The weather at 2015 for Timmins was wind 110° true (T) at 5 knots, visibility 8 statute miles in light rain with a broken ceiling at 500 feet above ground level (agl) and an overcast layer at 8000 feet agl, and a temperature of 18° C. There was no turbulence or conditions that might cause turbulence forecast for the time of the accident. These weather conditions may have been favourable for the formation of carburetor icing, but airframe icing was not forecasted for the time of the accident.
The weather reported near Horwood Lake at the approximate time of the accident was moderate rain and fog with a visibility of approximately 3 statute miles. The weather had been deteriorating since earlier in the evening. The end of civil twilight at the accident site was at 2029, and moonrise was not until 0218. The sky conditions and lack of moonlight would have reduced the sky luminousnessFootnote 7 to near darkness at the time C-GZFX departed the camp on Horwood Lake.
Aircraft
C-GZFX was a Robinson R44 (serial number 0595), a 4-place, single- engine (Lycoming O-540-F1B5, serial number L25387-40A) helicopter equipped with a 2-blade, articulated main rotor; a 2-blade, articulated tail rotor; and skid-type landing gear (Photo 1). The helicopter was certified with a maximum take-off weight of 2400 pounds and was equipped and certified for day flight under visual flight rules (VFR). A review of existing technical records indicated that it was equipped and maintained in accordance with existing regulations and approved procedures. There were no reported outstanding defects. The helicopter was originally certified for day and night VFR operations; however, C-GZFX did not have all of the required flight instruments on board to conduct night operations.

Operator
Apex Helicopters Inc. operates a commercial helicopter service under Subparts 702 and 703 of the Canadian Aviation Regulations (CARs). Operations conducted under Subparts 702 and 703 of the CARs require a minimum Type DFootnote 8 operational control system, which is generally used by smaller air operators that conduct short flights over an area close to the base of operations.
Under this type of operational control system, the operations manager delegates operational control of the flight (i.e., the decision to dispatch) to the pilot-in-command, but retains responsibility for all flight operations. Under this system, pilots are not normally required to consult with company supervisory personnel before dispatching from a base of operations.
Apex's company operations manual states that:
(2) When aircraft are in operation, a company representative knowledgeable with company flight operations will be on duty. If an occurrence occurs involving a company helicopter, He/she shall notify the Operations Manager or Chief Pilot by the quickest means available.Footnote 9
When the helicopter did not arrive at the FTC on the evening of 08 September, Apex was not informed.
Apex does not have a safety management system, nor is it required to do so under existing regulations.
Wreckage and impact information
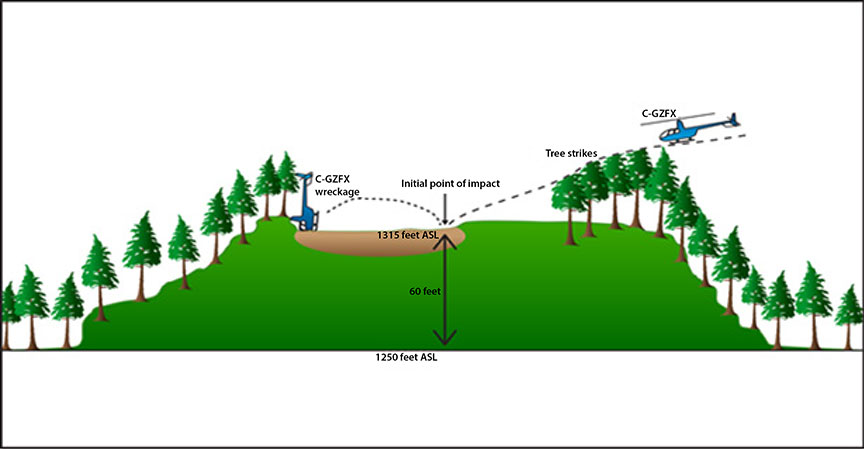
The wreckage site (Figure 3) was located at the top of a small hill that was approximately 65 feet higher that the surrounding terrain. The initial direction of the tree strike trail was 200° magnetic (M). The helicopter struck the ground in a sparsely treed area. The subsequent wreckage trail was approximately 30 feet long and lay in a direction of approximately 305°M. Ground scars and damage to the main rotor blades were indicative of high rotor torque at the time of impact. An inspection of the wreckage, including the main rotor system, tail rotor system, engine, and flight controls, did not reveal any pre-impact anomalies. The level of damage to the cockpit indicated that the impact with the ground was not survivable. The carburetor heat control was set to the “ON” position; therefore it is likely that carburetor icing did not affect the engine's performance.
Fuel recovered at the site indicated that the helicopter had approximately 144 pounds of fuel on board at the time of the accident and that the total occupant weight was approximately 360 pounds. The helicopter weighed approximately 2006 pounds at the time of the accident.
The fuel recovered from the helicopter at the wreckage site was tested and found to be free from contaminants. The wreckage was shipped to the TSB regional wreckage examination facility in Winnipeg, Manitoba, where the engine and major components were removed. The flight instruments and electronics were sent to the TSB Laboratory in Ottawa, Ontario. All of the flight instruments were badly damaged.
The engine was removed from the fuselage and taken to an engine repair facility, where accessory parts that had been damaged from the impact were removed and serviceable parts were installed. The engine was successfully started and run on an engine dynamometer under the guidance of TSB investigators. During testing, the engine performed within normal parameters, indicating that the engine was operating normally at the time of the accident.
Navigation
The helicopter was equipped with a VOR (very high-frequency omnidirectional range beacon) and an NDB (non-directional beacon). The pilot was known to have an application called Fore Flight installed on his cell phone, which, when coupled with a global positioning system (GPS) receiver/antenna,Footnote 10 would allow him to reference his position on a downloaded VFR chart, displayed on his cell phone or a tablet. It could not be determined if the pilot was using a GPS receiver or GPS-enabled cell phone to navigate.Footnote 11
Flight recorders
The helicopter was not equipped with a flight data recorder or a cockpit voice recorder, nor was either required by regulation, because the helicopter was configured with fewer than 10 seats.
Numerous TSB aviation investigation reports have referred to investigators being unable to determine the reasons an accident occurred due to the absence of on-board recording devices.Footnote 12 The benefits of recorded flight data in aircraft accident investigations are well known and documented.
In 2013, following its investigation into the March 2011 loss of control / in-flight break-up occurrence, northeast of Mayo, Yukon,Footnote 13, the TSB found that, if cockpit or data recordings are not available to an investigation, the identification and communication of safety deficiencies to advance transportation safety may be precluded. It further concluded that, if an accident does occur, recordings from lightweight flight recording systems would provide useful information to enhance the identification of safety deficiencies in the investigation. Therefore, the Board recommended that
the Department of Transport work with industry to remove obstacles to and develop recommended practices for the implementation of flight data monitoring and the installation of lightweight flight recording systems by commercial operators not currently required to carry these systems.
Transportation Safety Recommendation A13-01
The TSB assessed Transport Canada (TC)'s latest response to Recommendation A13-01 as follows:
In its response, TC has indicated proposed action in the form of an advisory circular to describe recommended practices regarding flight data monitoring programs. In addition, it will conduct focus group consultation to identify obstacles within TC's mandate and make recommendations for mitigation of those obstacles with respect to the installation of lightweight flight recording systems for commercial operators not required to carry these systems. The Board is encouraged by the intent of TC to work toward meeting the issues identified in the recommendation; however, the work is ongoing.
The response was assessed as Satisfactory Intent.Footnote 14
At the time of this occurrence, no steps had been taken by TC to require lightweight flight data and voice recorders to be installed on commercial helicopters that are configured with fewer than 10 seats.
Nighttime physiological factors
A number of hazards are associated with flying at night. These include a significant reduction in visual cues and potential sensory illusions that can lead to spatial disorientation.
The topography surrounding the accident site consisted of muskeg and bush that did not have any light or distinguishable features that could help a pilot identify a horizon. Darkness and the absence of visual cues make it more difficult to control and navigate an aircraft with reference to the ground, as well as to distinguish terrain and obstacles on the flight route.
The rules governing night flights are designed to reduce the risks associated with these challenges. Pilots flying visually (under VFR), for example, require strict weather and visibility minima as set out in the CARs. Pilots must also maintain “visual reference to the surface” at all times.Footnote 15 However, “visual reference to the surface” is not defined by the CARs. Any pilots flying over a dark, featureless landscape would have difficulty maintaining visual reference to the surface.
In May 2013, a Sikorsky S-76A helicopter crashed shortly after takeoff from Moosonee, Ontario, during hours of darkness.Footnote 16 To address the risks associated with this safety deficiency, the TSB issued Recommendation A16-08, which recommended that
Transport Canada amend the regulations to clearly define the visual references (including lighting considerations and/or alternate means) required to reduce the risks associated with night visual flight rules flight.
Transportation Safety Recommendation A16-08
Decision making
Decision making can be defined simply as the human process of gathering information, evaluating that information and then taking action based on that evaluation.
An important component of decision making is having good situational awareness, which requires a pilot to align the reality of a situation with his or her expectations. Inadequate or ineffective decision making can result in operating beyond an aircraft's capability or exceeding the pilot's abilities.Footnote 17 Some factors that can affect decision making include stress, fatigue, physical condition, attitude, and pressure (real or perceived). Perceived pressure is pressure that an individual places upon himself or herself, based on his or her perception of circumstances.
Emergency locator transmitters
The aircraft was equipped with a Kannad 406 Compact emergency locator transmitter (ELT). This type of ELT broadcasts signals on frequencies 406 megahertz (MHz) and 121.5 MHz. If the ELT is activated on impact or manually by the crew, the ELT transmits on both frequencies. The 406 MHz frequency is detected by a Search and Rescue Satellite-Aided Tracking (COSPAS-SARSAT)Footnote 18 satellite, which can transmit the downed aircraft's position to the JRCC in Trenton, Ontario. In this occurrence, the ELT activated upon impact; however, its antenna was shorn off during the impact sequence. It was transmitting a signal on both frequencies, but with the antenna being damaged, the 406 MHz signal was not received by the COSPAS-SARSAT satellite system, and neither frequency was detected by search and rescue aircraft.
In a 2009 report entitled Emergency Locator Transmitter (ELT) Performance in Canada from 2003 to 2008: Statistics and Human Factors Issues, Defence Research and Development Canada examined impact-related and human factors–related reasons for ELT failures during aircraft incidents. In total, the study determined that impact-related damage accounted for 92% of all failures among the occurrences that were examined. As a result, the report concluded that the “greatest opportunity for improvement is to address ELT failure due to crash impact.”Footnote 19 In particular, the report identified the following as possible areas for improvement:
- Crash impact survivability;
- Fire survivability;
- Survivability of connecting coaxial cable;
- Survivability of antenna; and
- Survivability and operation on submersion in water.Footnote 20
Emergency locator transmitter design and certification standards
According to CARs Part V – Airworthiness Manual, Chapter 551 – Aircraft Equipment and Installation, approved ELTs
must meet the performance and environmental standards of either:
(1) CAN-TSO-C91 or CAN-TSO-91a; or
(2) CAN-TSO-C126a.
In the case of a 406 MHz ELT, CAN-TSO-C126a states that new models must meet the qualification and documentation requirements in RTCA/DO-204A, Minimum Operational Performance Standards for 406 MHz Emergency Locator Transmitters (ELTs). RTCA /DO-204A states that ELT design “should provide a reasonable degree of crash survivability”Footnote 21 and be expected to survive a post-crash fire.Footnote 22
The aforementioned documents contain design criteria for maximum sustainable g loading,Footnote 23 aircraft mounting locations relative to the ELT unit itself, and some general guidelines regarding antenna location. However, they provide no specific guidelines on how to test existing and future units and how they might meet these standards and “provide a reasonable degree of survivability or survive a post-crash fire.”
A recent study conducted by the Canadian Mission Control Centre for SARSAT indicated that ELTs activate in only 38% of Canadian aircraft accidents where the aircraft sustained substantial damage. Studies conducted by other agencies, such as the Australian Transport Safety Bureau (ATSB) and the National Aeronautics and Space Administration (NASA) indicate ELT failure rates of up to 90%.Footnote 24,Footnote 25
SARSAT is currently involved in discussions with the International Civil Aviation Organization (ICAO) regarding a new design specification that will allow for intelligent ELTs that can determine when an emergency situation is inevitable and trigger the ELT prior to impact. There are also ongoing discussions concerning deployable ELTs (ELTs that are jettisoned from the aircraft prior to impact). At the time of report writing, these designs were in the conceptual stages at COSPAS-SARSAT, and no timeline for implementation had been projected.
As a result of TSB investigation A13H0001, the Board issued recommendations regarding ELT design and crashworthiness standards. The Board recommended that the International Civil Aviation Organization, the Radio Technical Commission for Aeronautics, the European Organisation for Civil Aviation Equipment, and the Department of Transport
establish rigorous emergency locator transmitter (ELT) system crash survivability standards that reduce the likelihood that an ELT system will be rendered inoperative as a result of impact forces sustained during an aviation occurrence.
Transportation Safety Recommendation A16-02, A16-03, A16-04, and A16-05
TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP218/2015 Instrument Examination
Analysis
General
A review of the technical records indicates that the helicopter was maintained in accordance with the air operator's maintenance control system and existing regulations. Prior to takeoff for the occurrence flight, there were no known technical difficulties with the helicopter. The investigation determined that there was nothing to indicate that the pilot's performance was degraded by fatigue or other physiological factors. The analysis will focus on decision making, spatial disorientation, the certification of ELTs and on-board flight recorders.
Decision making
When the pilot initially told the EACOM Timber Corporation supervisor that he would deliver the end-of-contract paperwork to the camp on Horwood Lake, the pilot's intention was to use the camp truck and drive it there. His text message to the 2 support personnel who were on their way to Timmins was sent to find out what time they would return the truck to the Foleyet Timber Camp (FTC). Upon learning that the crew would be late returning, the pilot took the helicopter. This was not a deviation from normal procedures, because Apex Helicopters Inc. operated under a self-dispatch system and because the pilot had left a flight itinerary at the camp.
However, a number of factors were present when the decision was taken to return to the FTC:
- The weather conditions had deteriorated.
- The flight departed under conditions of near darkness.
- The pilot did not have a night endorsement and was not instrument qualified, and he did not have adequate experience to undertake a flight in such conditions.
- The helicopter was not equipped for night visual flight rules (VFR) or instrument flight rules (IFR) operations.
These factors would have prevented the pilot from being able to determine his height above the forest canopy and to notice the rising terrain that lay ahead, and consequently the aircraft collided with the terrain.
The statement on the flight itinerary that the pilot would be back soon, along with the pilot's intention to depart the FTC early the next day for the ferry flight south, may have contributed to perceived pressure in the mind of the pilot.
Emergency locator transmitters
The ground crew at the FTC did not report the aircraft missing because they assumed the helicopter was staying at the Horwood Lake camp. When the helicopter crashed, the emergency locator transmitter (ELT)'s antenna was damaged and did not transmit a position report to the Joint Rescue Coordination Centre, Trenton. This delayed search and rescue operations until the helicopter was reported missing the next day.
The high rate of ELT failure indicates that existing ELT design and certification standards do not provide a reasonable degree of crash survivability.
If existing ELT design and certification standards do not ensure that the currently manufactured ELTs provide a reasonable degree of survivability from fire or impact forces, there is a risk that potentially life-saving search-and-rescue services may be delayed.
On-board flight recorders
Because current regulations do not require helicopters configured with fewer than 10 seats to be equipped with flight data or cockpit voice recorders, accident investigators will continue to have difficulty determining accident causes when other investigative information is not available. If cockpit and flight data recordings are not available to an investigation, this may preclude the identification and communication of safety deficiencies to advance transportation safety.
Findings
Findings as to cause and contributing factors
- The statement on the flight itinerary that the pilot would be back soon, along with the pilot's intention to depart the Foleyet Timber Camp early the next day for the ferry flight south, may have contributed to perceived pressure in the mind of the pilot.
- The flight was conducted in deteriorating weather and departed under conditions of near darkness. The pilot was not trained or certified for flight at night or in instrument conditions It is likely that the pilot was unable to determine his height above the forest canopy and to notice the rising terrain which lay ahead, and consequently the aircraft collided with the terrain.
- The ground crew at the Foleyet Timber Camp did not report the helicopter as being overdue, which contributed to the delay in search and rescue operations being initiated.
- The helicopter's emergency locator transmitter did not transmit its position on impact, which resulted in search and rescue operations being delayed by approximately 20 hours.
Findings as to risk
- If existing emergency locator transmitter design and certification standards do not ensure that the currently manufactured emergency locator transmitters provide a reasonable degree of survivability from fire or impact forces, there is a risk that potentially life-saving search-and-rescue services may be delayed.
- If cockpit and flight data recordings are not available to an investigation, this may preclude the identification and communication of safety deficiencies to advance transportation safety.
Safety action
Apex Helicopters Inc.
Since the accident, the operator has reviewed and emphasized the importance of timely reporting of overdue aircraft with all newly hired pilots and ground crew.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .