Loss of control and collision with water
Fort Langley Air Ltd.
Cessna 180H, C-FCDQ
Tyaughton Lake, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content.
History of the flight
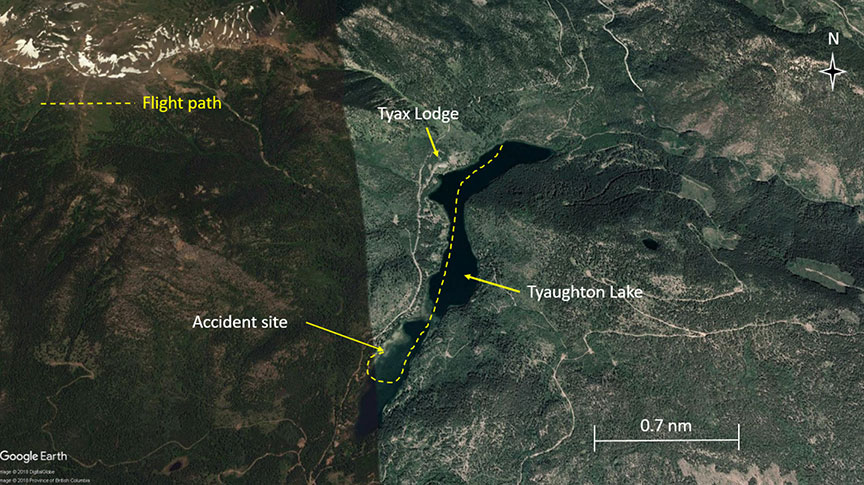
On 01 August 2018, following a local flight in the morning, the float-equipped Cessna 180H aircraft (registration C-FCDQ, serial number 18052166) (Figure 1) operated by Fort Langley Air Ltd. was refuelled. At approximately 1254,Footnote 1 the aircraft departed from Tyax Lodge on Tyaughton Lake, British Columbia, for a local sightseeing flight to take photographs, with 3 people on board. The pilot-in-command (the pilot) was seated in the front left seat, a passenger was seated in the front right seat, and another company pilot was seated in the rear left seat to provide local geographical knowledge.

Shortly after takeoff, while the plane was climbing through approximately 300 feet, the other company pilot observed fuel leaking from the left wing and communicated that information to the pilot. The other company pilot reportedly told the pilot to turn around and return to land on the lake. Given the local terrain, the pilot reduced the airspeed and banked the aircraft steeply to the right, turning back toward the lake. The aircraft then abruptly rolled further to the right and struck the lake in a near-vertical attitude at approximately 1255 (Figure 2). The aircraft was substantially damaged on impact and sank.
The investigation was unable to determine whether the emergency locator transmitter activated; however, even if it had activated, it is unlikely that the signal would have been detected because the transmitter was immersed in water. A local resident on the shore called 911 and initiated the rescue operation. The company pilot in the rear seat and the passenger were fatally injured,Footnote 2 and the pilot-in-command sustained serious injuries.
The pilot-in-command and the passenger had been wearing the available lap belt and shoulder harness. The other company pilot had been wearing the available lap belt; no shoulder harness was available in the rear seat. Although personal flotation devices were available in the aircraft during the occurrence flight, none of the occupants were wearing them, nor were they required to by regulation. The aircraft was not equipped with exits that allowed for rapid egress, nor were such exits required by regulation.
Weather information
The Environment and Climate Change Canada weather observation station closest to Tyaughton Lake is located at Pemberton Airport (CYPS), British Columbia, 38 nautical miles to the south. The conditions recorded at 1300 were a temperature of 32.3 °C and a dew point of 14.1 °C.
A local report described the weather conditions at Tyaughton Lake at the time of the accident as clear skies, wind between 9 and 11 km/h from the south-southeast, temperature 24.8 °C, dew point 12.2 °C, and a pressure setting of 30.03 inHg.
The operating density altitude at Tyaughton Lake was calculated at 5250 feet above sea level, based on the temperature, dew point, and pressure setting.
Density altitude
An aircraft operating at a higher density altitude, as opposed to at sea level, travels at a higher true airspeed while maintaining the same indicated airspeed. A higher true airspeed increases the aircraft's turn radius. Therefore, the aircraft's true airspeed and turn radius are directly proportional to density altitude. In a level, coordinated turn, there would be about a 15% larger turn radius at a density altitude of 5250 feet above sea level, compared to a turn at sea level in standard-day conditions, when flown at the same indicated airspeed and bank angle.
Pilot information
Pilot-in-command
Records indicate that the pilot-in-command was certified and qualified for the flight in accordance with existing regulations. He had received a seaplane rating on 22 April 2018, obtained a commercial pilot licence – aeroplane on 26 June 2018, and held a valid Category 1 medical certificate. The pilot had accumulated a total of 287.9 flight-time hours, including 98.4 hours on floatplanes. Of the total flight-time hours, 132.7 hours were as pilot-in-command, including 60.7 hours as pilot-in-command on the Cessna 180H.
Based on a review of the pilot's work–rest schedule, fatigue was not considered a factor in the accident.
The pilot had not received egress training, nor was it required by regulation.
The other company pilot
The other company pilot had obtained a commercial pilot licence – aeroplane on 26 May 2016 and received a seaplane rating on 29 January 2017. He had accumulated a total of approximately 800 flight-time hours, including an estimated 360 hours on floatplanes. He was hired by the company as a charter pilot and seaplane instructor on 01 May 2017. He had provided the pilot-in-command of the occurrence aircraft approximately 20 hours of instruction toward his seaplane rating.
Aircraft information
The Cessna 180H float-equipped aircraft has a maximum take-off weight of 1338 kg (2950 pounds). The occurrence aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. It had no known deficiencies and was being operated within its weight and balance and centre-of-gravity limits. The aircraft was not equipped with a flight data recorder, nor was it required to be by regulation.
Accident site and wreckage information
Tyaughton Lake is approximately 3300 feet above sea level. The aircraft struck the lake in a near-vertical attitude and came to rest inverted, in 10 to 15 feet of water about 50 feet from shore, with the floats partially above the water (Figure 3).

The majority of the wreckage was located near the fuselage. Both floats had severe damage to the tips and showed impact damage resulting from the contact with the water. All of the control surfaces were accounted for. An examination of the flap system indicated that the flaps were in the 20° position at the time of impact. All damage to the airframe was attributable to impact forces. The fuel selector was found to be set to both tanks, which contained sufficient fuel for the remainder of the flight. The left fuel cap had not been replaced after refuelling and was found hanging from its chain. Damage to the engine and propeller were consistent with a high power setting at the time of impact.
The aircraft's flight instruments were severely damaged. The global positioning system (GPS) and SPOT Satellite GPS Messenger were removed from the aircraft and sent to the TSB Engineering Laboratory in Ottawa, Ontario, for further examination. The GPS unit did not provide any usable flight profile data.
Accelerated stall
The airspeed at which a stall occurs is related to the load factor of the manoeuvre being performed. In straight and level flight, lift is equal to weight, and the load factor is 1g. However, in a banked level turn, greater lift is required. One way to achieve lift is by increasing the angle of attack (by pulling back on the elevator control), which increases the load factor. As the load factor increases with bank angle, there is a corresponding increase in the speed at which the stall occurs. As a result, steep turns are often accomplished with the addition of engine power to maintain or increase airspeed.
A stall that occurs as a result of a high load factor, such as bank angle greater than 30°, is called an accelerated stall. Accelerated stalls, which occur at higher airspeeds due to the increased load factor on the wing, are usually more severe than unaccelerated stalls and are often unexpected. For example, a stall from a 60° to 70° bank angle will result in rapid departure from controlled flight and a significant loss of altitude before recovery is possible.
The occurrence aircraft was equipped with a stall warning system, but no warning was heard during the flight. The functionality of the system could not be tested due to the damage to the aircraft.
The occurrence aircraft had a Horton STOL-CraftFootnote 3 kit installed, which included the following modifications to the aircraft: full Camber-Lift leading edges on both wings, stall fences on the top of the wings, droop wing tips, and aileron gap seals. Although Horton does not publish actual demonstrated stall speeds, the supplemental type certificate does indicate that the “stall speeds, takeoff performance and landing performance are equal to or better than the performance of the unmodified airplane.”Footnote 4 According to the manufacturer, when the Horton STOL kit is installed, “on average you can expect to get a 4-7 knot reduction in stall speeds.”Footnote 5
In this occurrence, after reportedly being told by the other company pilot to turn and land on the lake, the pilot-in-command began a tight turn, which resulted in a loss of control and the impact with the water.
TSB recommendations relating to seaplanes
The TSB has issued several recommendations with respect to seaplane operations to eliminate or reduce safety deficiencies that pose significant risks. The following sections provide highlights of some of those recommendations.
Recommendation on rapid egress exits
During the investigation into an accident involving a DHC-2 departing Lyall Harbour, British Columbia, in 2009,Footnote 6 the TSB recognized the importance of having exits available from which persons inside a sinking aircraft can escape, and recommended that
the Department of Transport require that all new and existing commercial seaplanes be fitted with regular and emergency exits that allow rapid egress following a survivable collision with water.TSB Recommendation A11-05
In January 2017, Transport Canada (TC) responded to Recommendation A11-05 by indicating that, in 2006, it had conducted an evaluation of egress from submerged seaplanes, which included suggestions to enhance safety, but concluded that there was no readily identifiable design solution that would have a major impact on the existing level of floatplane safety. TC indicated that it would therefore focus on regulatory requirements for egress training and other enhancements on floatplane safety, and would not devote further activity to Recommendation A11-05.
The March 2017 reassessment of TC's response states that the intent of the TSB recommendation is to reduce the risk of occupants being trapped when some or all exits are jammed, as a result of an accident.
Emergency door release mechanisms, better door handles, and push-out windows have been developed for certain types of floatplanes. Although some floatplane operators have installed these modifications, many have not.
Regulatory requirements for mandatory egress training for commercial floatplane pilots may result in some improvement in emergency egress from commercial seaplanes. However, if the regulator does not mandate or promote voluntary modifications to normal exits, seaplanes will continue to operate with exits that could become unusable following an impact, diminishing the occupants' chances to exit the aircraft following a survivable accident.
Therefore, the response to Recommendation A11-05 was last assessed as Satisfactory in Part.
Recommendations on personal flotation devices and egress training
Following the Lyall Harbour accident in 2009, the TSB also recognized that if a personal flotation device is not worn, and in the absence of other rescue capabilities, there is a higher risk that survivors of water impact will drown.
The TSB recommended that
the Department of Transport require that occupants of commercial seaplanes wear a device that provides personal flotation following emergency egress.TSB Recommendation A11-06
In addition, the TSB has recognized, after many seaplane accidents, that pilots who receive underwater egress training have a greater chance of escaping the aircraft and surviving an accident. Those pilots can then help passengers to safety. In 2013, following a DHC-2 floatplane accident in Lillabelle Lake, Ontario,Footnote 7 the TSB recommended that
the Department of Transport require underwater egress training for all flight crews engaged in commercial seaplane operations.TSB Recommendation A13-02
Both of these recommendations (A11-06 and A13-02) have led to proposed regulatory changes that were published in the Canada Gazette, Part I, on 21 May 2016. With regard to Recommendation A11-06, the regulations would require all commercial seaplane occupants to wear a flotation device while boarding the seaplane, and while it is operated on or above water. The regulatory changes would also introduce mandatory underwater egress training for pilots of commercially operated seaplanes, with recurrent training every 3 years, which addresses Recommendation A13-02.
While TC had initially indicated that the proposed regulatory changes would be published in the Canada Gazette, Part II, in 2017, TC's latest response now states that it anticipates the changes to be published in Part II in fall 2018. As of the date of publication of this report, no proposed regulatory changes have been published. The Board is concerned about the additional delay of the publication of these amendments in the Canada Gazette, Part II. Although these amendments will, if published as currently proposed, substantially reduce or eliminate the safety deficiency identified in recommendations A11-06 and A13-02, until they are fully implemented, the risks to transportation safety remain.
Therefore, the responses to recommendations A11-06 and A13-02 were assessed as showing Satisfactory Intent.
Safety messages
Pilots must pay particular attention to the aircraft's airspeed and bank angle when manoeuvring at low altitudes. When pilots manoeuvre at high bank angles, the airspeed at which an aircraft will stall is higher than in wings-level flight, and the pilot may not expect the early onset of the accelerated stall.
As density altitude increases, so does the radius of a turn. Pilots must recognize that an increased density altitude affects aircraft performance and turning radius.
Pilots-in-command are ultimately responsible for aircraft handling.
None of the aircraft's occupants were wearing a personal flotation device, the pilot did not have underwater egress training, and the aircraft was not equipped with exits that allowed for rapid egress, nor were any of these required by regulation. In this occurrence, the close proximity of the accident site to the shoreline enabled a quick response and the rescue of the pilot.
Safety action taken
Following this accident, Fort Langley Air Ltd. made several changes to its training program. These changes included the following:
- increased awareness and training on fuelling procedures and the importance of confirming that fuel caps are replaced after fuelling;
- increased awareness and training on procedures and action to be taken if a fuel cap is found to have been left off while the aircraft is in flight; and
- awareness and understanding of cockpit distraction.
This concludes the TSB's limited-scope investigation into this occurrence. The Board authorized the release of this investigation report on . It was officially released on .