Power loss and loss of control in flight
Aries Aviation International
Piper PA-31, C-FNCI
Calgary/Springbank Airport, Alberta, 40 nm SW
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content.
Summary
On 01 August 2018, after completing 2 hours of survey work near Penticton, British Columbia (BC), an Aries Aviation International Piper PA-31 aircraft (registration C-FNCI, serial number 31-8112007) proceeded on an instrument flight rules flight plan from Penticton Airport (CYYF), BC, to Calgary/Springbank Airport (CYBW), Alberta, at 15 000 feet above sea level. The pilot and a survey technician were on board. When the aircraft was approximately 40 nautical miles southwest of CYBW, air traffic control began sequencing the aircraft for arrival into the Calgary airspace and requested that the pilot slow the aircraft to 150 knots indicated airspeed and descend to 13 000 feet above sea level. At this time, the right engine began operating at a lower power setting than the left engine. About 90 seconds later, at approximately 13 500 feet above sea level, the aircraft departed controlled flight. It collided with terrain near the summit of Mount Rae at 1336 Mountain Daylight Time. A brief impact explosion and fire occurred during the collision with terrain. The pilot and survey technician both received fatal injuries. The Canadian Mission Control Centre received a 406 MHz emergency locator transmitter signal from the occurrence aircraft and notified the Trenton Joint Rescue Coordination Centre. Search and rescue arrived on site approximately 1 hour after the accident.
Factual information
History of the flight
The International Civil Aviation Organization's Annex 13 requires states conducting accident investigations to protect cockpit voice recordings. Footnote 1 Canada complies with this requirement by making all on-board recordings privileged under the Canadian Transportation Accident Investigation and Safety Board Act. While the Transportation Safety Board (TSB) may make use of any on-board recording in the interests of transportation safety, it is not permitted to knowingly communicate any portion of an on-board recording that is unrelated to the causes or contributing factors of an accident or to the identification of safety deficiencies.
The reason for protecting on-board recordings lies in the premise that these protections help ensure that pilots will continue to express themselves freely and that this essential material is available for the benefit of safety investigations. The TSB has always taken its obligations in this area very seriously and has vigorously restricted the use of on-board recording data in its reports. Unless the on-board recording is required to both support a finding and identify a substantive safety deficiency, it will not be included in the TSB's report.
To validate the safety issues raised in this investigation, the TSB has made use of the available on-board recording in its report. In each instance, the material has been carefully examined in order to ensure that it is required to advance transportation safety.
An Aries Aviation International (Aries Aviation) Piper PA-31 aircraft (registration C-FNCI, serial number 31-8112007) was deployed to the Okanagan valley, BC, on 18 July 2018 for survey activities, consisting of flying over selected areas at 3600 feet above the highest terrain at a ground speed of 150 knots. For each flight, a survey equipment technician sat in the cabin of the aircraft and operated the various pieces of equipment for the survey, and the pilot sat in the front left seat of the cockpit. Each survey mission averaged 6 hours of flight time and was typically conducted between 0800 and 1600 local time.
On 01 August 2018, the aircraft departed Penticton Airport (CYYF), BC, at 1026 Footnote 2 with full fuel Footnote 3 and began survey operations at 1034, to the east of CYYF. The survey portion of the flight lasted for 2 hours, with the aircraft being flown at 10 000 feet for the final hour. Footnote 4 Once the survey was completed, the pilot airfiled an instrument flight rules flight plan to Calgary/Springbank Airport (CYBW), Alberta. Air traffic control (ATC) issued a clearance for the pilot to climb to and maintain an altitude of 15 000 feet and to proceed directly to the IGVEP waypoint (Figure 1).

During the climb through 11 000 feet, the autopilot was selected ON, and the pilot switched the fuel selectors from INBOARD to OUTBOARD. Shortly after the aircraft reached 15 000 feet, at 1256, the pilot selected the fuel pumps ON, in accordance with the aircraft flight manual (AFM), Footnote 5 and left them ON for the rest of the flight. The autopilot altitude hold (ALT) mode was selected. The pilot then assisted the survey technician in activating the portable oxygen system. Two minutes later, the pilot put an oxygen mask up to his face, and, a few seconds later, he put it down.
At 1328, the autopilot ALT mode disengaged. Over the following 47 seconds, the aircraft started to climb from an altitude of 15 000 feet, assigned by ATC, Footnote 6 to 15 400 feet. It then started a descent, reaching a peak vertical speed of 3200 fpm and an acceleration of 0.5g. Footnote 7 After 9 seconds of descent, the pilot levelled off at 15 000 feet (with an acceleration of 1.7g) and engaged the ALT mode.
At 1330:55, ATC instructed the pilot to descend to 14 000 feet. At 1331, the pilot switched the fuel tanks from the OUTBOARD to the INBOARD position, in accordance with the AFM, Footnote 8 selected pitch mode on the autopilot, and began the descent to 14 000 feet. The aircraft entered cloud during the descent and levelled off at 14 000 feet 90 seconds later, at which point ALT mode was selected.
At 1333, ATC asked the pilot for his indicated airspeed (IAS), but the pilot read back the altitude of 14 000 feet. ATC, once again, asked for the IAS, but this time the pilot read back the ground speed of 170 knots instead; the actual IAS was 140 knots. ATC then asked the pilot to slow to 150 knots indicated airspeed (KIAS) and to descend to 13 000 feet.
A few seconds later, the manifold pressure (MP) on both engines decreased, which resulted in the left-hand MP gauge indicating an MP of 18 inches of mercury (inHg) and a fuel flow of 22 U.S. gallons per hour, and the right-hand engine indicating an MP of 15 inHg and a fuel flow of 14 U.S. gallons per hour.
After the power reduction, the autopilot ALT mode disengaged. The navigation and pitch mode, as well as the flight director mode, remained ON. The aircraft's airspeed decreased to below the single-engine inoperative best rate-of-climb speed (VYSE) of 97 KIAS, Footnote 9 and the aircraft maintained an altitude of 13 900 feet. The airspeed reached 91 KIAS, and the stall horn began to sound intermittently. The IAS began to increase as the MP for the left engine increased to 34 inHg with a fuel flow of 38 U.S. gallons per hour. At the same time, the right MP gauge indicated 20 inHg and a fuel flow of less than 10 U.S. gallons per hour. The aircraft began a brief descent, and the airspeed increased to 100 KIAS.
At 1334:40 the aircraft deviated to the right (south) of the intended track, and its altitude decreased to 13 500 feet. The aircraft then began to climb, and the IAS began to decrease below VYSE once again. At 1335:43, ATC called the pilot to confirm that he was going to the IGVEP waypoint. The stall warning horn was sounding continuously at this time. The pilot replied that there was a problem with the right engine. Shortly afterward, the airspeed decreased to 71 KIAS, and the aircraft departed controlled flight and went into a right-hand spin (Appendix A).
The aircraft exited the clouds at 13 300 feet. Shortly afterward, the engine fuel-flow monitors indicated idle fuel flow, or about 4.5 U.S. gallons per hour, for each engine. Commensurate with the power reduction and decrease in airspeed, the rpm of both engines decreased. When the right engine reached 700 rpm, the right-alternator failure (R ALT INOP) warning light illuminated on the annunciator panel, followed immediately by both the left- and right-pneumatic-source failure (L PNEU INOP and R PNEU INOP) warning lights. As the airspeed increased to 110 KIAS in the spin, the rpm of both engines also increased. When the aircraft reached 110 KIAS, the right-alternator failure warning light went out, followed by the right and then the left pneumatic-source failure warning lights.
As the aircraft descended through 11 500 feet, ATC asked the pilot to report his situation. The pilot declared an emergency. The aircraft continued spinning, and, during the spin, the pilot occasionally input full left and partial right aileron on the control column. The aircraft did not recover from the spin. It completed 7.5 revolutions before colliding with terrain at 10 000 feet, near the peak of Mount Rae, at 1336:17.
Injuries to persons
Table 1. Injuries to persons
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | 1 | 1 | – | 2 |
| Serious | 0 | 0 | – | 0 |
| Minor/None | 0 | 0 | – | 0 |
| Total | 1 | 1 | – | 2 |
The impact forces were not survivable, and all injuries were related to the nature of the impact.
Damage to aircraft
The aircraft collided with steep, rocky terrain in a near-vertical nose-down attitude. The aircraft was destroyed, with both wings and both engines broken off from the fuselage. The wreckage trail was approximately 900 feet long, and the main portion of the fuselage came to rest on a snowy, icy slope.
Other damage
Not applicable.
Personnel information
| Pilot licence | Airline transport pilot licence (ATPL) |
|---|---|
| Medical expiry date | 01 June 2019 |
| Total flying hours | 4400 |
| Flight hours on type | 2800 |
| Flight hours in the last 7 days | 41 |
| Flight hours in the last 30 days | 41 |
| Flight hours in the last 90 days | 135 |
| Flight hours on type in the last 90 days | 135 |
| Hours on duty prior to the occurrence | 5.6 |
| Hours off duty prior to the work period | 14.0 |
The pilot had started flying in 1999. After obtaining his commercial pilot licence in 2002, he flew for a variety of flight schools and air-taxi operators. In 2007, he started training for his multi-engine instrument rating, which he obtained in 2009. At the time of the accident, the pilot's licence and instrument rating were valid and current in accordance with the Canadian Aviation Regulations (CARs).
In 2012, the pilot was hired by Aries Aviation, and, in 2015, he obtained his airline transport pilot licence. Survey flying at Aries Aviation is done primarily in visual meteorological conditions, and instrument flying is limited to training or transiting to and from the work area. From the information collected during the investigation, the pilot's flight time in instrument meteorological conditions could not be determined.
Based on the review of the information available pertaining to the pilot's work–rest cycle, fatigue was not a factor in this occurrence.
Aircraft information
| Manufacturer | Piper Aircraft, Inc. |
|---|---|
| Type, model, and registration | PA-31 Navajo, C-FNCI |
| Year of manufacture | 1981 |
| Serial number | 31-8112007 |
| Certificate of airworthiness/flight permit issue date | 03 November 2006 |
| Total airframe time | 7277.4 hours |
| Engine type (number of engines) | Lycoming TIO-540-A2C (2) |
| Propeller/Rotor type (number of propellers) | Hartzell HC-E3YR-2ATF (2) |
| Maximum allowable take-off weight | 6840 pounds |
| Recommended fuel type(s) | 100/130 minimum-grade aviation gasoline |
| Fuel type used | 100LL aviation gasoline |
Records indicate that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. Before this occurrence, the aircraft had been operating for 10 days without any reported problems. The aircraft was equipped with a BLR Aerospace LLC vortex generator kit that had been installed in accordance with Supplemental Type Certificate Footnote 10 SA00047SE. The kit consisted of 86 vortex generators of different sizes installed on the wings and on the vertical stabilizer, as well as 4 strakes (2 on each nacelle). The supplemental type certificate also provided for an increase in gross take-off weight from 6500 pounds to 6840 pounds. Additionally, the markings on the airspeed indicator were changed to reflect the change in performance for the aircraft.
When the aircraft departed Penticton, it weighed approximately 6885 pounds (45 pounds over the gross take-off weight) and was within the forward and aft limits of the centre of gravity envelope. When the aircraft departed controlled flight, it weighed approximately 6000 pounds, and its weight and centre of gravity were within the prescribed limits.
Performance charts from the AFM indicate that the single-engine service ceiling Footnote 11 at the time of the accident was 16 500 feet. At 13 500 feet, the single-engine climb rate at 97 KIAS is 350 fpm.
Automatic flight control system
The aircraft was equipped with a Bendix King KFC 200 automatic flight control system with a flight director. The system consists of a 2-axis autopilot, an electric pitch trim system, and a flight director indicator, which provides pitch and roll commands on a v-bar display system integrated with the captain's attitude indicator.
The autopilot can operate in several vertical and lateral modes, including ALT mode, heading select mode, navigation mode, and approach mode. Supplement 8 in the PA-31 AFM identified the following steps to take if the autopilot is engaged during an engine failure:
- Disengage AP [autopilot]
- Follow basic Airplane Flight Manual single-engine procedures.
- Airplane rudder and aileron axes must be manually trimmed prior to engaging autopilot for single-engine operations. Footnote 12
In addition, the supplement provided the following caution:
When the autopilot is engaged, manual application of a force to the pitch axis of the control wheel for a period of three seconds or more will result in the autotrim system operating in the direction to create a force opposing the pilot. This opposing mistrim force will continue to increase as long as the pilot applies a force to the control wheel and will ultimately overpower the autopilot. If the autopilot is disengaged under these conditions, the pilot may be required to exert control forces in excess of 50 pounds to maintain the desired aircraft attitude. The pilot will have to maintain this control force while he manually retrims the aircraft. Footnote 13
Single-engine emergency procedures
The Aries Aviation Standard Operating Procedures for the PA-31 state that pilots must maintain a minimum speed of VYSE; if the power cannot be restored to a failed engine, they must complete the ENGINE FAILURE IN FLIGHT checklist and land as soon as practical at the nearest suitable airport. The ENGINE FAILURE IN FLIGHT checklist is as follows:
ENGINE SECURING PROCEDURE..... COMPLETE
AIRSPEED..... VYSE MINIMUM
COWL FLAPS (OPERATING ENG)..... AS REQUIRED Footnote 14
The ENGINE SECURING procedure requires the following actions to be completed from memory:
CONTROL..... MAINTAIN DIRECTION AND AIRSPEED
MIXTURES..... FORWARD
PROPELLERS..... FORWARD
THROTTLES..... FORWARD
LANDING GEAR..... RETRACT
FLAPS..... RETRACT
FUEL BOOST PUMPS..... ON
INOPERATIVE ENGINE..... IDENTIFY
THROTTLE (IN-OP ENG..... RETARD TO VERIFY
PROPELLER (IN-OP ENG..... FEATHER
MIXTURE (IN-OP ENG.)..... CUTOFF Footnote 15
Spin recovery
The AFM for the PA-31 and the Aries Aviation Standard Operating Procedures do not describe spin-recovery procedures for the PA-31, nor are such descriptions required by regulation. There are no certification requirements to demonstrate spins in a multi-engine aircraft. However, Transport Canada advises the following spin-recovery procedure for small aircraft if no data are available from the manufacturer. Footnote 16 In summary, the steps are to
- Close the throttles/power to idle
- Neutralize the ailerons
- Apply full opposite rudder to the direction of the spin
- Move the control column briskly forward
- Maintain these control inputs until rotation stops
- Neutralize rudder
- Recover from the resulting dive
Aircraft oxygen system
The aircraft was originally fitted with a factory-installed oxygen system. This system had been disabled when Aries Aviation leased the aircraft, and a Scott portable oxygen system was made available for flight crew use. The Scott model 5500 portable oxygen system consisted of an oxygen tank–regulator assembly Footnote 17 of 1800 psi and 38.4 cubic feet, and 2 facemasks Footnote 18 with connecting plastic tubing. The facemasks cover both the mouth and nose but do not include a microphone to interface with the aircraft's intercom system. To don the mask, a pilot has to remove the headset, put on the mask, and put the headset back on—two hands are required to don the mask effectively—and continue communications with the mask in between the boom microphone of the headset and his or her mouth.
In the occurrence aircraft, the tank and facemasks were in a plastic carrying case located behind the front right seat. The oxygen tank had been filled on 19 July 2018. During the impact sequence, the oxygen tank pressure gauge was sheared off, releasing any oxygen that remained in the tank. The shut-off valve on the tank regulator was found in the OPEN position.
Meteorological information
At the time of the accident, there was a weak low-pressure system over the southern border between BC and Alberta, centred west of Red Deer, Alberta. An upper trough oriented north-to-south over the central portion of Alberta was moving eastward at 15 knots. The graphical area forecast Footnote 19 for the area near the accident site called for a few clouds, based at 12 000 feet and up to 14 000 feet. Isolated thunderstorms were forecast for the area northwest of CYBW after 1400. The freezing level was forecast to be at approximately 12 500 feet.
Observed weather at the location and time of the accident was consistent with the forecast. A broken layer of cumulus clouds based at 13 000 feet was prevalent, with no significant wind or turbulence. A few hours after the accident, there were thunderstorms near CYBW. The digital engine monitor in the aircraft recorded an outside air temperature of −2 °C at 14 000 feet. Information from the Appareo Systems Vision 1000 (see section 1.11.2 of this report) did not record any in-flight icing, severe turbulence or thunderstorm conditions.
Aids to navigation
Not applicable.
Communications
Not applicable.
Aerodrome information
Not applicable.
Flight recorders
General
The aircraft was not equipped with a traditional flight data recorder or a cockpit voice recorder, nor was either required by regulation. However, the aircraft was equipped with 2 devices (an Appareo Systems Vision 1000 and a J.P. Instruments Engine Data Monitor 790) that provided significant information about the flight path and engine performance.
The TSB determined that, because the Appareo System Vision 1000 was installed in the occurrence aircraft such that it was not intended to be controlled by the operating personnel on the flight deck of the aircraft, the recorded images and voice communications were privileged in accordance with the Canadian Transportation Accident Investigation and Safety Board Act. Footnote 20
The flight path data, audio files, and image files retrieved from the Appareo system enabled the investigators to better understand the underlying factors that contributed to the accident.
Appareo Systems Vision 1000
Aries Aviation installed an Appareo Vision 1000 flight data monitoring (FDM) system in the occurrence aircraft on 12 March 2018. The unit is a self-contained flight data recording system that only requires a power and ground lead from the aircraft's electrical system to operate. The information captured by the Vision 1000 includes the following:
- Attitude data (pitch, roll, yaw, etc.)
- WAAS [wide area augmentation system] GPS [global positioning system] (latitude, longitude, ground speed, vertical speed, GPS altitude, etc.)
- Cockpit imaging
- Ambient audio
- Intercom system audio for crew and ATC communications (optional) Footnote 21
When the system was originally installed and set up in the aircraft, the imaging provided by the camera included the entire left side of the instrument panel, the entire centre instrument panel, and the power-lever quadrant. The FDM system was installed using installation data for the Cessna model 172, and the electrical provisions were installed using data from the U.S. Federal Aviation Administration's Advisory Circular 43.13-1B. Footnote 22 The installation included an optional intercom system for crew and ATC communications.
After the initial installation, the Appareo unit had been bumped into inadvertently, which altered the recorded field of vision. In addition, the pitch information recorded by the unit was now inaccurate. At the time of the accident, only the 4 engine instruments Footnote 23 at the top of the centre instrument panel were visible, along with a portion of the left instrument panel, and a significant view out the cockpit windshields. Because the power-lever quadrant was no longer being recorded by the FDM system, the investigation was unable to determine the positions of both engine controls just before and during the accident sequence.
The Vision 1000 unit in the occurrence aircraft was damaged during the impact, but all 8 GB of data were recovered, including audio and images for the last 2.6 hours of the flight, as well as 200 flight hours of inertial data.
The TSB Engineering Laboratory in Ottawa, Ontario, analyzed the data from the Appareo to assess the aircraft's performance during the occurrence. The following is a summary of the performance from the start of the asymmetrical power condition to the loss of control.
The aircraft continued along course, with a small left bank angle. As the airspeed decreased toward 86 KIAS, the aircraft rolled to the right, up to about 20°, and entered a shallow right-hand turn, before it began descending again. The bank angle approached wings level momentarily, before returning to about 20° right. When the airspeed subsequently increased toward 100 KIAS, the right bank angle decreased toward wings level.
The increasing right roll with reduced airspeed, and the decreasing right roll with increasing airspeed, may indicate reduced lateral directional control at low airspeed, with asymmetric power. Unfortunately, the flight control inputs are unknown, as is the level of turbulence that may have been encountered. The minimum control speed in the air (known as VMCA) published in the AFM is 76 KIAS (with flaps in take-off position).
When the aircraft subsequently pitched up to about 20°, the airspeed decreased at a rate of about 3 knots per second in the resulting climb. Although the airspeed dropped to 75 KIAS, (1 knot below the minimum control speed in the air), the bank angle remained briefly at 5° to 10° to the right. At 75 KIAS, with increased power on the left engine, the lateral directional control would be expected to degrade more significantly.
While the aircraft was still pitched at a 20° nose-up angle, it ceased climbing and the airspeed decayed to 73 KIAS. The high angle of attack associated with this flight condition suggests that the wing may have stalled. The level-flight stall speed for a clean configuration published in the AFM is about 74 KIAS at 6000 pounds. The aircraft was 1 knot below this speed.
The published stall speed is for idle power, which appears consistent with the right-engine power level at the moment of the upset. The left engine, however, had considerable power, and its prop wash would tend to delay stall on the left wing. Therefore, the right wing would be expected to stall first, which would result in the aircraft rolling and yawing to the right.
Engine data monitor
The aircraft was equipped with a JPI EDM-790 engine-data analyzer. The analyzer, containing non-volatile memory, was recovered from the aircraft and sent to the TSB Engineering Laboratory in Ottawa, Ontario, for data download and analysis. The data recovered consisted of the following parameters for both engines:
- Exhaust-gas temperature (EGT) at the turbocharger
- EGT for each cylinder
- Cylinder-head temperature for each cylinder
- Fuel flow
- Oil temperature
- Outside air temperature
The analysis of these data found that a significant fuel flow discrepancy (split) between the left-hand and the right-hand engines had started on 08 July 2018. Before this date, the fuel flows were fairly evenly matched between both engines (within a couple of gallons per hour). Further analysis of the data found that the right-hand engine fuel-flow information was representative of the actual operating conditions. A review of the aircraft's maintenance records did not indicate any maintenance actions that would have caused this discrepancy.
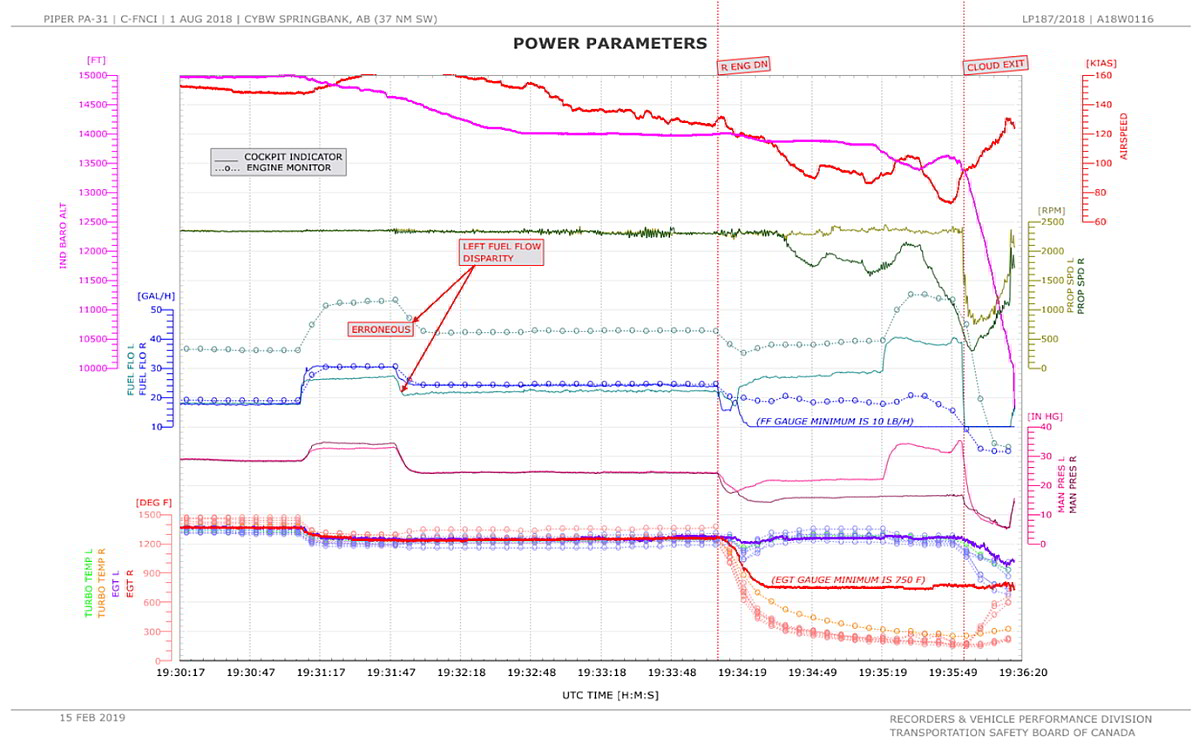
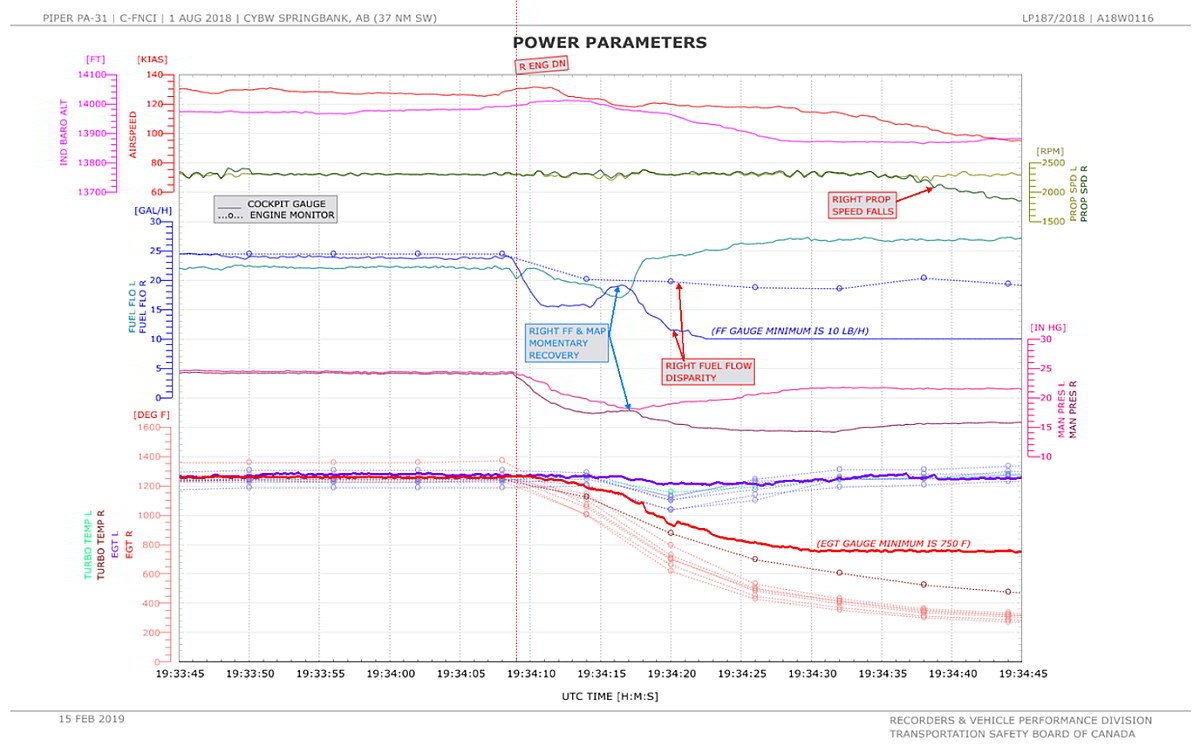
The TSB Engineering Laboratory examined the engine parameter data in support of the aircraft performance analysis. The following is a summary of the observations from the engine data Footnote 24 from the beginning of the power asymmetry and the loss of control.
On the day of the occurrence, before 1334:09, the parameters of the engines were well matched. The largest difference was in the indicated fuel flow (FFI), with the right engine's flow being higher than the left engine's flow by about 2 to 3 U.S. gallons per hour (approximately 10%).
After 1334:09, the FFI and indicated manifold pressure (MPI) of both engines began decreasing; however, the right-engine flow fell more quickly (Appendix B). Furthermore, the indicated right-engine exhaust-gas temperature (EGTI) and the recorded right-engine exhaust-gas temperature (EGTR) began to decrease, whereas, in the left engine, these parameters remained relatively steady.
Within 10 seconds, the right-engine FFI and MPI increased momentarily. The right-engine FFI then fell toward the minimum levels (the gauge minimum being 10 U.S. gallons per hour), and the right-engine MPI fell to about 15 inHg. At the same time, the left-engine FFI and MPI increased.
Unlike the right-engine FFI, the right-engine recorded fuel flow (FFR) did not fall toward minimum levels, remaining between 18 and 20 U.S. gallons per hour. (It had been about 24 U.S. gallons per hour before the drop in power level.) This disparity between the right-engine FFI and FFR generally continued until the end of the flight. FFI is measured at the fuel servo by a direct reading pressure gauge calibrated in U.S. gallons per hour. FFR is measured by a vane-type fuel-flow sensor installed between the engine driven fuel pump and the fuel servo.
In consultation with the manufacturer of the engine data monitor, the investigation determined that the most likely explanation for a sudden disparity in fuel-flow readings between the two systems is air being introduced into the engine fuel supply. As the viscosity of an air–fuel mixture is significantly lower than that of aviation gasoline alone, it flows through the fuel supply system faster, accounting for the higher FFRreading.
The left-engine FFI then increased to higher levels than before the drop in power level (27 versus 22 U.S. gallons per hour), and the left-engine MPI increased but was still slightly lower than before the drop in power level (22 inHg versus 24 inHg).
When the airspeed dropped below 110 KIAS, the right-propeller rpm began to fall below 2300.
Wreckage and impact information
Approximately 95% of the wreckage was recovered from the accident site and shipped to the TSB regional office in Edmonton, Alberta, for further examination. The flight control system was examined, and no pre-impact anomalies were noted. The landing gears were in the retracted position, and the flaps were in the up position.
The aircraft fuel system was examined to the degree possible. The left and right fuel-tank selectors were found in the INBOARD position. The right-hand nacelle-tank fuel cap was tested for water leaks; none were observed. The inboard fuel-tank caps were also tested for water leaks, and it was noted that some water (about 2.5 mL per hour) was seeping by the O-ring gaskets, which were cracked and aged.
TSB personnel, along with a representative from the manufacturer, examined the right-hand engine. None of the components from the fuel, air, or ignition systems that were recovered and examined indicated any faults that would have prevented the engine from developing rated power.
Medical and pathological information
Nothing of note was found in the post mortem examination. There was nothing in the pilot's medical history that would indicate a predisposition to sudden incapacitation.
Fire
A brief impact explosion and fire occurred during the collision with terrain. The fire was extinguished by the time the aircraft came to rest. Superficial burn damage and soot were noted around the engines, nacelles, and inboard wing sections.
Survival aspects
There were at least 11 witnesses, and several of them called 911. The aircraft's 406 MHz emergency locator transmitter activated. The Canadian Mission Control Centre received the signal, and search and rescue arrived on site approximately 1 hour after the accident. The accident was not survivable owing to the impact forces.
Tests and research
TSB laboratory reports
The TSB completed the following laboratory report in support of this investigation:
- LP187/2018 – Flight path analysis
Organizational and management information
Aries Aviation is authorized to conduct aerial work and air-taxi operations under Subpart 702 and Subpart 703, respectively, of the Canadian Aviation Regulations (CARs). On 07 September 2017, the company was issued an operations specification to conduct aerial surveying in North America under Subpart 702 of the CARs in day and night visual flight rules and in instrument flight rules (VFR, IFR, and night VFR) conditions. The specification also provided for the carriage of persons. Footnote 25
Additional information
Oxygen regulations and hypoxia awareness
The use of oxygen is necessary to prevent and relieve in-flight oxygen deprivation (hypoxia). Upon use, individuals will often return to a normal functioning state, although the speed and degree of recovery depend on how severely hypoxic they were. Continued use of supplementary oxygen is required at altitude to avoid returning to a hypoxic state.
Section 605.31 of the CARs stipulates that, for unpressurized aircraft such as the occurrence aircraft, a supply of oxygen be available for the flight crew and at least 1 passenger for flights exceeding 30 minutes at cabin-pressure altitudes above 10 000 feet but not exceeding 13 000 feet. When the aircraft is operating at cabin-pressure altitudes above 13 000 feet, a supply of oxygen must be available for all persons.
In addition, section 605.32 of the CARs states the following regarding the use of oxygen:
(1) Where an aircraft is operated at cabin-pressure-altitudes above 10,000 feet ASL [above sea level] but not exceeding 13,000 feet ASL, each crew member shall wear an oxygen mask and use supplemental oxygen for any part of the flight at those altitudes that is more than 30 minutes in duration.
(2) Where an aircraft is operated at cabin-pressure-altitudes above 13,000 feet ASL, each person on board the aircraft shall wear an oxygen mask and use supplemental oxygen for the duration of the flight at those altitudes. Footnote 26
The Aries Aviation Company Operations Manual Footnote 27 reiterates the requirements of section 605.31 of the CARs.
Aries Aviation requires pilots to take recurrent theoretical training on high-altitude physiology every 3 years. The pilot's most recent training was on 19 July 2018. Theoretical training includes awareness of physiology in low-pressure environments, including respiration and hypoxia; other factors associated with rapid loss of pressurization, such as cabin temperature change and noise; and required actions. Transport Canada Footnote 28 requires this training only for pilots operating pressurized aircraft above 13 000 feet.
Some commercial and most military pilots also get the opportunity to experience the effects of hypoxia (for example, in hypobaric chambers), to familiarize themselves with how hypoxia may affect them individually. Such practical training is important to demonstrate how insidious hypoxia is and how a pilot continues to feel normal while progressively being unable to reliably perform certain tasks. Aries Aviation did not provide the occurrence pilot with such practical training, nor was the company required to do so by regulation. At the time of writing, Simon Fraser University in BC offers the only high-altitude physiology course in Canada Footnote 29 that offers hypobaric chamber training to civilians.
Hypoxia
As explained in Ernsting's Aviation and Space Medicine, “Normoxia describes the state in which a physiologically adequate supply of oxygen to the tissues, whether in quantity or molecular concentration, is available. When the level of oxygen available is below that requirement, a state of hypoxia is said to exist.” Footnote 30 There are different types of hypoxia, all of which involve different mechanisms of oxygen deprivation. Hypoxic hypoxia is the most common type related to flight; it can occur in flight above certain altitudes, because “as barometric pressure falls, breathing ambient air will result in a fall of the partial pressure, and thus the molecular content, of the oxygen in the lung.” Footnote 31 This results in individuals experiencing a “reduction in the oxygen tension in their inspired gas” Footnote 32 and, ultimately, has a detrimental effect on their associated performance.
However, the severity and onset of hypoxia vary, depending on a multitude of factors. The altitude and onset rate affect hypoxia. For example, ascending slowly to 13 000 feet may produce a slow onset of symptoms; however, rapid decompression at 30 000 feet can be fatal within minutes. The effects of hypoxia also vary depending on personal conditions such as individuals' health and fitness and their use of medications or alcohol, as well as on the activity or task(s) the individuals are engaged in and how significantly the activity affects their respiration rate.
- Various scientific studies have highlighted the typical symptoms of hypoxia, but results vary depending on participant characteristics, the test environment, and the actual test conducted. Because of variability in research results, as well as the factors described above, it is impossible to accurately assign a cause-and-effect value to a specific altitude. However, typical effects on human physiology and performance of an ascent from 7000 feet to 15 000 feet without supplementary oxygen include the following: Physiological responses. In a resting person, “ascent to an altitude of 10 000 feet [above sea level] produces a fall in the partial pressure of oxygen in the lung alveoli but only a slight fall in the percentage saturation of haemoglobin with oxygen”, Footnote 33 but above 10 000 feet, “the percentage saturation of haemoglobin falls quickly.” Footnote 34 Thus, for a period of time at this altitude, the body's physiology initially compensates for the change in oxygen pressure. However, the heart rate increases by a small percentage immediately when breathing air at an altitude above 6000 to 8000 feet and by about 10% to 15% at 15 000 feet, with an associated rise in systolic blood pressure and a shift in blood distribution, for example, away from the skin and toward the heart and brain. Footnote 35 Above 15 000 feet, normal physiological mechanisms no longer offer compensatory protection, and a pilot may start to experience headache, dizziness, “air hunger” (gasping for air), and fatigue. Footnote 36
-
Performance detriments. The brain normally uses a substantial amount of oxygen and, therefore, is very susceptible to a reduction in oxygen pressure. As altitude increases, there is a gradual degradation in thinking, memory, judgment, muscular coordination, and reaction time. Footnote 37 Hearing decreases and peripheral vision narrows as the visual field darkens. Specifically, novel tasks are the most difficult to carry out, and even learned and practised tasks become more challenging to execute. Footnote 38
Once a pilot reaches around 15 000 feet, performance detriments will become more pronounced for more demanding tasks, such as manual flying or emergency handling, which requires conceptual reasoning, use of short- or long-term memory, decision making, critical judgment, quicker reaction time, and/or hand–eye coordination with muscular coordination. In fact, by 15 000 feet, a pilot may experience restrictions to the visual field, a 25% decrement in memory capacity, and a decrement in hand–eye coordination of 20% to 30% with fine tremors in the hand, making it more and more difficult to hold a control in a fixed position. A pilot's ability to judge airspeed, heading, and orientation, as well as to deal with in-flight emergencies, becomes progressively more impaired around this altitude. Footnote 39
- Inability to detect hypoxic symptoms. Although certain hypoxia effects may become more noticeable than others as an aircraft ascends, associated changes to a pilot's sense of self, motivation, willpower, and wellness often overshadow the ability to identify performance degradation in themselves. In fact, a pilot who is in a hypoxic state may actually experience euphoria. Even sensory effects, such as darkening of the visual field, may become noticeable to individuals only after they begin to revert to normal (i.e., after using oxygen or descending to a lower altitude). Footnote 40
Respiration, hypoxia, and hyperventilation
As explained in Human Performance and Limitations in Aviation, “The most powerful stimulus to respiration is caused by the body's perception of an increase in carbon dioxide tension, rather than it's [sic] perception of a reduction in the oxygen tension in the blood.” Footnote 41 As a pilot ascends, his or her respiration rate may therefore increase. However, a pilot may end up eliminating too much carbon dioxide (without breathing in adequate oxygen supplies), and the hypoxia may subsequently lead to hyperventilation, a condition in which individuals' increased respiration rate causes them to exhale more than they inhale.
Other symptoms of hyperventilation include lightheadedness, dizziness, tingling, and, potentially, spasms and contractions in the extremities. Footnote 42 Some hypoxia studies have also noted that it is not always clear whether these effects are due to hypoxia or to the associated hyperventilation. Aviation medicine texts also advise that, if pilots experience hyperventilation, they should suspect hypoxia as an initiating condition. Footnote 43
Anxiety and stress can also lead to an increase in respiration rate and hyperventilation. Footnote 44 Although these can occur in any pilot, hypoxic pilots may be more likely than others to experience stress and anxiety situationally, for example, upon perception of difficulties with task performance. If an individual starts to hyperventilate, the rapid breathing often produces more anxiety, resulting in an uncontrolled cycle unless intervention occurs. A pilot may therefore be vulnerable to hyperventilation if he or she is hypoxic and may be especially vulnerable if he or she is both hypoxic and stressed.
During the in-flight emergency in this occurrence, the pilot's breathing rapidly changed to short, sharp, and quick respirations.
Analysis
The aircraft's systems were examined, in an attempt to explain the power loss in the right engine and to identify issues that would have prevented the pilot from recovering from the spin. These examinations were as detailed as possible but were limited owing to the extensive breakup of the aircraft upon impact with the mountain. The examinations and tests performed did not reveal any condition or failure that would have prevented the right engine from producing rated power. Furthermore, the flight control system did not exhibit any conditions that would have led to the loss of control or would have prevented the aircraft from recovering from the spin.
The weather information collected during the investigation identified that the loss of control was not due to in-flight icing, thunderstorms, or turbulence.
The analysis will discuss the effects of hypoxia, the possible reasons for the power loss, the loss of control, and the pilot's inability to recover from the spin.
Hypoxia and performance degradation
The pilot likely experienced some degree of hypoxia in this occurrence. Based on the results of controlled research on hypoxia in humans, the investigation concluded that, during the ascent to and continued flight at 15 000 feet without supplementary oxygen, the occurrence pilot may have experienced headache, dizziness, air hunger, and fatigue, as well as gradual degradations in thinking, memory, judgment, and muscular coordination. His reactions would also have slowed down. His hearing capacity may have started to decrease, and his peripheral vision may have narrowed as the visual field darkened. The pilot may have found it more and more difficult to perform tasks using working memory or to judge airspeed, heading, and orientation. However, due to the slow and gradual onset of symptoms and the probable associated sense of well-being, it is unlikely these effects were noticeable to the pilot.
While the aircraft was at 15 000 feet, the autopilot altitude hold mode disengaged and the aircraft ascended to 15 400 feet, 400 feet above the cleared altitude. The pilot did not immediately respond to this involuntary ascent. When he did respond, his response was unusually aggressive. A few minutes later, air traffic control (ATC) requested the pilot's indicated airspeed. After a delay, the pilot responded with an altitude reading. ATC requested his indicated airspeed again, but the pilot responded with the ground speed this time. This performance could be indicative of degradations in thinking, memory and judgment, and more specifically of difficulty with working-memory tasks due to hypoxia.
The pilot did not continuously use oxygen above 13 000 feet and likely became hypoxic as the aircraft climbed to and maintained an altitude of 15 000 feet. The pilot did not recognize his symptoms or take action to restore his supply of oxygen, resulting in degradation of his ability to manage normal flying tasks in an effective and timely manner.
To maintain situational awareness during the asymmetric flight condition and to respond appropriately to this condition, the pilot needed to perceive the critical elements of the flight environment and comprehend quickly what they meant. Although the engine gauge parameters differed between left and right engines, the airspeed decreased, the heading changed, and the aircraft deviated from the intended track, there were no aural or visual cautions or warnings of an engine-power loss. The aircraft more or less maintained its course and airspeed during this initial stage of the emergency.
The rapid increase in the pilot's breathing indicates that the pilot may have realized that something was wrong; however, his response was slow and inappropriate. Specifically, the response to the asymmetric power condition was delayed, and the memory-based tasks associated with the single-engine emergency checklist were not performed.
As a result of hypoxia-related cognitive and perceptual degradations, the pilot was unable to maintain effective control of the aircraft or to respond appropriately to the asymmetric power condition.
Hypoxia and oxygen use
The pilot's high-altitude training included several hours of theoretical training. In this occurrence, the pilot used the oxygen system intermittently. However, the pilot did not have practical training experience that would have allowed him to familiarize himself with how hypoxia might affect him specifically. Such practical training is important to demonstrate how hypoxia results in a progressive degradation of performance although the pilot may feel normal.
If flight crews do not undergo practical hypoxia training, there is a risk that they will not recognize the onset of hypoxia when flying above 13 000 feet without continuous use of supplemental oxygen.
Asymmetric power and loss of control
When the pilot was instructed to reduce speed and subsequently descend, power was reduced for both engines. It is not known which actions the pilot actually took; however, the responses of the aircraft (reduction in indicated airspeed, yaw/course change towards the right, and reduced fuel flow) indicate that the right-engine power decreased more than the left. The reason for the reduction in power on the right engine and subsequent power asymmetry could not be determined.
Because the Appareo camera had been bumped and its position changed, the pilot's actions on the power controls could not be determined. Therefore, the investigation was unable to determine whether the power asymmetry was the result of power-quadrant manipulation by the pilot or of an aircraft system malfunction.
The right-engine fuel flow recorded by the digital engine monitor remained much higher than the indicated fuel flow on the cockpit gauge. The tests on the right-engine fuel system did not reveal any mechanical reason for a loss of fuel flow. The most likely explanation for a sudden disparity in fuel flow reading between the two systems is air introduced into the engine fuel supply. As the viscosity of an air–fuel mixture is significantly lower than that of aviation gasoline alone, it flows through the fuel supply system faster, accounting for the increase in the fuel flow recorded by the digital engine monitor. Additionally, it would also account for the reduction in the indicated fuel flow on the cockpit gauge, which was due to a reduction in fuel pressure at the fuel servo.
The aircraft departed controlled flight and entered a spin to the right because the airspeed was below both the published minimum control speed in the air and the stall speed, and because there was a significant power asymmetry, a high angle of attack, and significant asymmetric drag from the windmilling propeller of the right engine.
When the aircraft exited cloud, the pilot completed only 1 of the 7 spin-recovery steps: reducing the power to idle. As the aircraft continued to descend, the pilot took no further recovery action, except to respond to ATC and inform the controller that there was an emergency.
Findings
Findings as to causes and contributing factors
- The pilot did not continuously use oxygen above 13 000 feet and likely became hypoxic as the aircraft climbed to 15 000 feet. The pilot did not recognize his symptoms or take action to restore his supply of oxygen.
- As a result of hypoxia-related cognitive and perceptual degradations, the pilot was unable to maintain effective control of the aircraft or to respond appropriately to the asymmetric power condition.
- The aircraft departed controlled flight and entered a spin to the right because the airspeed was below both the published minimum control speed in the air and the stall speed, and because there was a significant power asymmetry, a high angle of attack, and significant asymmetric drag from the windmilling propeller of the right engine.
- When the aircraft exited cloud, the pilot completed only 1 of the 7 spin-recovery steps: reducing the power to idle. As the aircraft continued to descend, the pilot took no further recovery action, except to respond to air traffic control and inform the controller that there was an emergency.
Findings as to risk
- If flight crews do not undergo practical hypoxia training, there is a risk that they will not recognize the onset of hypoxia when flying above 13 000 feet without continuous use of supplemental oxygen.
Other findings
- The weather information collected during the investigation identified that the loss of control was not due to in-flight icing, thunderstorms, or turbulence.
- Because the Appareo camera had been bumped and its position changed, the pilot's actions on the power controls could not be determined. Therefore, the investigation was unable to determine whether the power asymmetry was the result of power-quadrant manipulation by the pilot or of an aircraft system malfunction.
- The flight path data, audio files, and image files retrieved from the Appareo system enabled the investigators to better understand the underlying factors that contributed to the accident.
Safety action
Safety action taken
Aries Aviation International
Aries Aviation International purchased individual cannula-style oxygen masks for each of its pilots.
In addition, the Company Operations Manual was updated with a statement that all crew members shall use oxygen continuously at cabin altitudes above 10 000 feet and any time below 10 000 feet to enhance performance or reduce fatigue.
The following changes were made to the training program:
- Annual training will have a greater focus on oxygen use.
- Use of a PA-31 flight simulator will be gradually phased in to eventually expose flight crew to a training practice every 6 months.
- Management will schedule field visits during survey work.
- Training will be enhanced for both pilots and maintenance engineers in response to the overall decrease in workforce experience in the aviation industry.
This report concludes the Transportation Safety Board of Canada's investigation into this occurrence. The Board authorized the release of this report on 17 July 2019. It was officially released on 01 August 2019.
Appendices
Appendix A – Final flight path of the aircraft leading up to the loss of control and spin entry (looking toward the southeast)
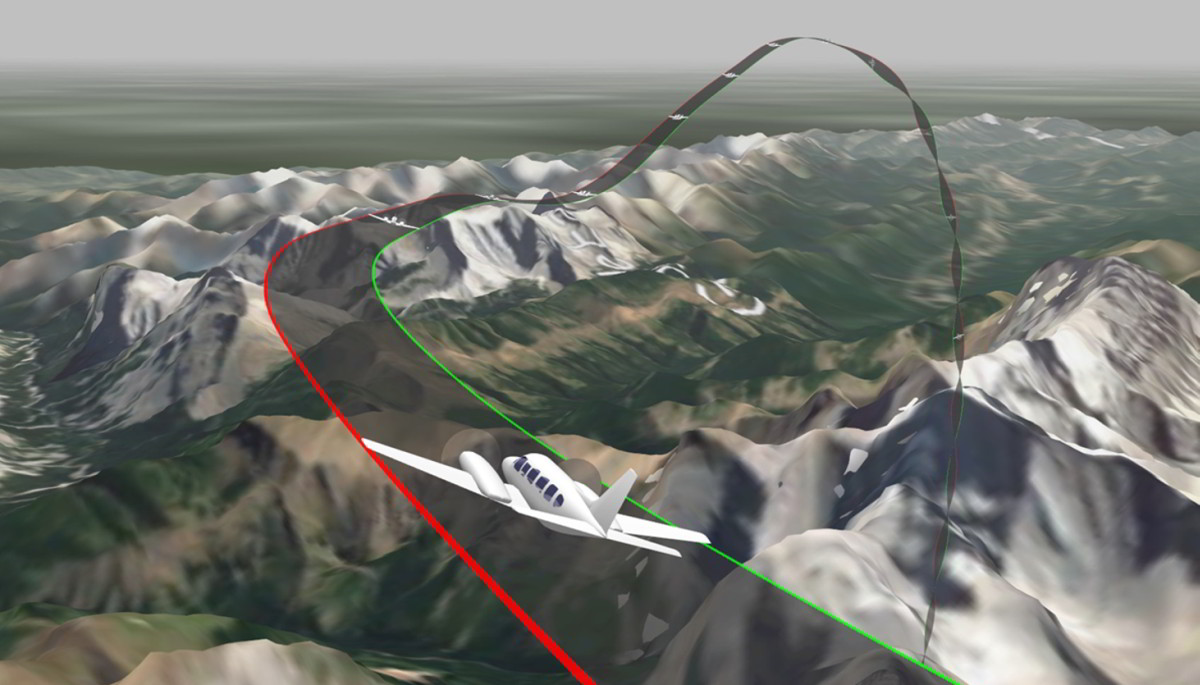
Source: Appareo system data
Appendix B – Power parameters from the Appareo system and the digital engine data monitor