Grounding
Bulk carrier Tundra
Sainte-Anne-de-Sorel, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content.
Summary
On 28 November 2012, the bulk carrier Tundra departed Montréal, Quebec, under the conduct of a pilot, downbound in the St. Lawrence River for Halifax, Nova Scotia. At approximately 2148 Eastern Standard Time, the vessel exited the navigation channel and ran aground off Sainte-Anne-de-Sorel, Quebec. The vessel was refloated on 05 December. No pollution or injuries were reported; however, the vessel sustained minor damage.
Factual information
Particulars of the vessel
| Name of vessel | Tundra |
|---|---|
| IMO number | 9415208 |
| Port of registry | Limassol |
| Flag | Republic of Cyprus |
| Type | Bulk carrier |
| Gross tonnage | 19 814 |
| LengthFootnote 1 | 185.0 m |
| Draught at departure | Forward: 8.36 m Aft: 8.39 m |
| Built | 2009, Weihai Shipyard, China |
| Propulsion | 1 six-cylinder diesel engine (7200 kW) driving a single fixed propeller |
| Cargo | 19 533 metric tons of soya beans |
| Crew members | 18 |
| Registere downer | Prehniet Beheer B.V. (Geldrop, Netherlands) |
| Manager | S.A. Navarone (Amaroussion, Greece) |
Description of the vessel
The Tundra is a bulk carrier with machinery and accommodation spaces located aft (Photo 1). The vessel has 6 cargo holds that are serviced by 3 electric-hydraulic cranes mounted on the vessel's centreline. Each crane has a lifting capacity of 30 tonnes.

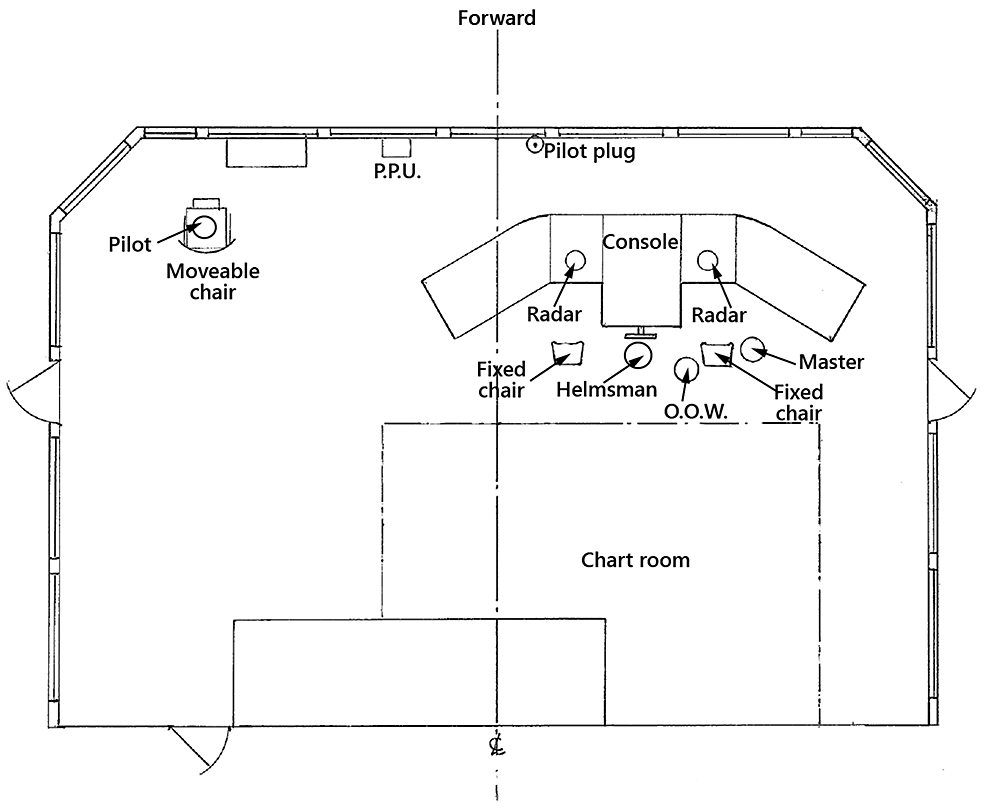
The bridge console is located slightly starboard of the vessel's centreline and consists of a conning position, engine controls, and 2 fixed chairs (Appendix A). The navigation chart table and Global Maritime Distress Safety System station are located aft of the bridge console. The bridge is equipped with the required navigational equipment, including 3 cm and 10 cm radars located in front of both the port and starboard fixed chairs.
Montréal/Trois-Rivières pilotage sector
At 1430Footnote 2 on 28 November 2012, a pilot from the Corporation des Pilotes du Saint-Laurent Central (CPSLC)Footnote 3 was assigned by the Laurentian Pilotage Authority (LPA) to navigate the Tundra from Montréal to Trois-Rivières, a trip of approximately 6 hours covering a distance of 66 nautical miles (nm). Pilotage is compulsory by regulation in this sector due to the difficulties and hazards involved in navigating the river. The navigation channel, with a minimum depth of 11.3 m and minimum width of 229 m,Footnote 4 is marked throughout by range lights and buoys, most of which are lit. These buoys are either removed or replaced with spar buoys by the Canadian Coast Guard (CCG) prior to the winter navigation season.
On 23 October 2012, the CCG announced the beginning of the first phase of the fall buoy program via Notice to Shipping (NOTSHIP) Q1632 that stated the mooring of winter buoys and lifting of summer buoys was in progress in the Québec region. The NOTSHIP further indicated that the appropriate Marine Communication Traffic Services (MCTS) Centre could be contacted for more information concerning the buoy program. Information pertaining to the CCG's seasonal buoy program was available on the regular CCG marine broadcasts and on the CCG Central and Arctic region website.Footnote 5
Events prior to departure
In the 3 days prior to the occurrence, the pilot had been assigned to pilot 2 vessels upbound from Trois-Rivières to Montréal. One assignment was on 25 November, during his 10 scheduled days off, and the other was on 27 November, his first day back to work. On 28 November, at 1430, he was assigned to pilot the Tundra from section 50 in the Port of Montréal to Trois-Rivières. The vessel was scheduled to leave at 1830 that same day, bound for the Port of Halifax en route to Hamburg, Germany.
When the pilot embarked at 1815, a master-pilot exchange took place and the following items were discussed: navigation equipment, steering gear type, propeller type, direction of propeller rotation, and bow thruster type/capacity. The pilot completed the pilot card and examined the wheelhouse poster. He set up his portable pilotage unit, which was loaded with navigational software, on the port side of the bridge and connected it to the vessel's automatic identification system unit. Prior to departure, the Tundra's bridge team had developed a passage plan that was handed over to and signed by the pilot. The vessel's passage plan was not discussed during the master-pilot exchange. The pilot's passage plan was not shared with the bridge team.
History of the voyage
At 1830 on 28 November, the Tundra departed Montréal in good visibility under the conduct of the pilot. The master, the helmsman, and the second officer acting as officer of the watch (OOW) were on the bridge along with the pilot. As the vessel proceeded downbound in the St. Lawrence River, the pilot primarily used navigational buoys to monitor its progress and make course alterations. Both the pilot and OOW monitored the vessel's progress independently of one another, and the pilot made use of his mobile phone for personal phone calls and text messages. Exchanges of information between the pilot and the bridge team were minimal.
At 2000, the bridge team did a watch change, and both the OOW and the helmsman were replaced. The third officer, who was now acting as OOW, monitored the vessel's progress by using the differential global positioning system to plot the vessel's position (latitude and longitude) on the paper navigation chart prior to each waypoint.Footnote 6 He then recorded the date and time of the plotted positions in the list of pre-established waypoints on the vessel's passage plan.
At approximately 2136, the vessel was proceeding at a speed of 14.5 knotsFootnote 7 and the pilot ordered that the course be altered to 083° true (T) (Figure 1). The helmsman repeated the order and executed the manoeuvre, which put the vessel in line with the range lights on Île du Moine. The pilot then sat in a moveable chair on the port side of the bridge, approximately 8 m away from the other members of the bridge team (Appendix A).
The next course was 052°T,Footnote 8 and the pilot's passage plan included an intermediat course of 060°T that was to be initiated when buoy S-140Footnote 9 was abaft of the vessel (Figure 1). However, buoy S-140 had been removed 7 days earlier as part of normal CCG operations, and the next lateral buoy on the port side was S-136.Footnote 10 The vessel's passage plan did not include the intermediate course; it indicated the next course change (waypoint No. 63) as being 0.44 nm downriver of buoy S-140's announced position,Footnote 11 at the intersection of courses 083°T and 052°T (Figure 1).
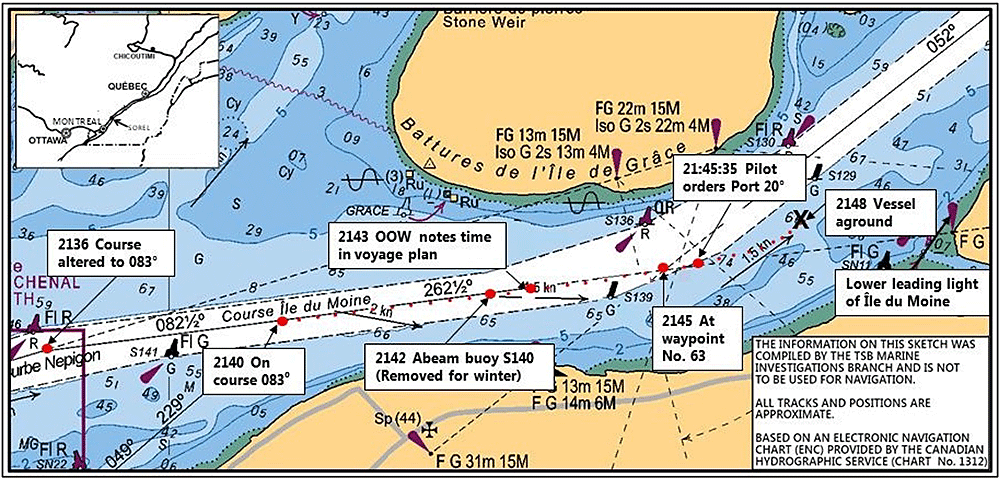
At 2142, the vessel passed abeam of buoy S-140's announced position and continued on course 083°T (Figure 1). No additional helm orders were issued by the pilot, who remained seated on the port side of the bridge. At 2143, 2 minutes before the vessel reached waypoint No. 63, the OOW logged the time and date in the list of pre-established waypoints on the vessel's passage plan. At 2144:54,Footnote 12 the vessel passed waypoint No. 63, at which point it became more difficult for the helmsman to maintain the course of 083°T due to bank effectFootnote 13 as the vessel began to exit the navigation channel.
At 2145:20, the helmsman stated that the wheel was at starboard 20° and that the vessel was not responding to helm. The pilot abruptly asked for clarification, and the helmsman repeated that he could not steer. The pilot stood up and went to the middle of the wheelhouse to look out the bridge front window. Although there had been no change to the engine control setting, by 2145:35, the vessel's speed had reduced to 12.9 knots. At this time, the pilot ordered the rudder 20° to port. The helmsman repeated and executed the order, but the vessel did not turn in response to the rudder action. The pilot then ordered hard to port. The helmsman carried out the order, but the vessel's response was minimal. Approximately 30 seconds later, the vessel's heading was 071°T and its speed was 11.5 knots. The pilot ordered a course of 050°T and then ordered the wheel amidship. At 2148, the vessel was aground in position 46°04.0′ N, 073°02.17′ W (Figure 1). Immediately following the grounding, the pilot ordered full astern to the OOW, who executed the manoeuvre. The engine action had no effect and the vessel remained aground. The pilot then contacted MCTS Québec to report the grounding.
Refloating of the vessel
On 01 December, an initial attempt to refloat the vessel with 4 tugs was made, but it was unsuccessful. On 03 December, 1717 metric tons of cargo was unloaded and 4 tugs were used in a second unsuccessful attempt to refloat the vessel. On 05 December, after an additional 925 metric tons of cargo was unloaded, the vessel was successfully refloated with the assistance of 4 tugs, at which time it proceeded under its own power to Trois-Rivières. Upon arrival, an underwater inspection was carried out; the vessel then reloaded its cargo before departing for Halifax at 1730 on 06 December.
Damage to the vessel
The underwater survey report for the Tundra identified the following:
- scratches and an indent at frame 132
- a slight buckle in 1 propeller blade
- 1 inspection cover missing from the starboard side of the rudder.
Environmental conditions
At 2200 on 28 November 2012, the air temperature was 0.6°C and the wind was from the NNE at a speed of 30 km/h. The vessel's records indicated good visibility, clear weather, and a water temperature of 3°C. Canadian Hydrographic Service chart 1312 indicated the current off Sainte-Anne-de-Sorel to be 1.5 knots in an easterly direction.
Vessel certification
The Tundra was certified and equipped in accordance with existing regulations.
Personnel certification and experience
Themaster, officers, and crew were properly certified for their positions on board. The master had received training in bridge resource management (BRM) and had acted as master on numerous vessels since 2002. He had occupied this position on the Tundra since 28 August 2012. The OOW had been sailing on the Tundra since 25 August 2012, the date he joined the vessel. He had sailed on other vessels since 2000. The helmsman had been sailing since 2006 and had joined the vessel on 20 November 2012.
The pilot held a Master Intermediate Voyage certificate of competency issued on 03 March 1991. He was hired as an apprentice pilot by the LPA in 1996 and obtained a Class C licence for the Montréal to Trois-Rivières sector in 1998. In 2003, he upgraded to a Class A licence, which allowed him to pilot vessels of any size within this sector.
Bridge resource management
BRM is the effective management and use of all resources, both human and technical, available to the bridge team to ensure the safe completion of a voyage. BRM includes concepts such as workload management, problem-solving, decision-making, and teamwork. Situational awareness and communication are key to BRM; specifically, bridge team members have a responsibility to maintain overall situational awareness as well as be responsible for their individual duties.
Situational awareness
Situational awareness is used to describe an individual's awareness and comprehension of operational conditions and contingencies.Footnote 14 In maritime pilotage operations, effective situational awareness involves 1) perceiving critical factors in the environment, 2) understanding what those factors mean with respect to controlling the vessel, and 3) projecting what will happen within the near future and taking appropriate action.
Communication
The international language used in maritime operations is English. The pilot's first language was French. The Tundra's crew was Ukrainian and heir working language was Russian. During the voyage, the bridge team communicated in English.
Cultural factors can play a role in communication and hence the effectiveness of BRM. “Power distance” refers to the extent to which members of a culture feel comfortable with hierarchy and power imbalance in personal and business relationships. Research has shown that cultures vary in terms of power distance.Footnote 15 Compared to low power distance cultures, high power distance cultures are more comfortable with imbalance among their members, which means that people in less powerful positions may be reluctant to question or challenge authority figures.Footnote 16 Cultural differences in power distance may contribute to poor communication between marine pilots and bridge teams.Footnote 17 The National Transportation Safety Board recommends that a segment on cultural and language differences and their possible influence on mariner performance be included in the International Maritime Organization (IMO)'s BRM curricula.Footnote 18
Bridge resource management training requirements
As of 01 January 2005, the General Pilotage Regulations require all licensed marine pilots and marine pilot applicants in Canada to hold a certificate of attendance from a BRM training program. The Convention onStandards of Training, Certification and Watchkeeping of Seafarers (STCW) and 2010 Manila Amendments require a demonstration of BRM competencies and knowledge in order for seafarers to obtain a watchkeeping mate certificate and require BRM training in order to obtain a master's certificate.
While the LPA requires its pilots to undergo BRM training, there are no guidelines, procedures, or assessments to ensure pilots implement BRM best practices on board. The pilot had received BRM certification as part of his ongoing pilot training in 2001 and again in 2008. There is no indication that the OOW on the Tundra was certified in BRM.
Passage planning and monitoring
Under IMO Resolution A.893(21), voyage planningFootnote 19 is a required task obliging the development of a plan in accordance with IMO rules and other factors specified by the master. The vessel's passage plan is intended to enhance safety by highlighting high-risk areas and providing key information in a format that is readily available to those involved in the vessel's navigation. When a pilot boards a vessel, it is important that both the vessel's passage plan and the pilot's passage plan are discussed during the master-pilot exchange. The pilot's passage plan is normally complex and consists of numerous landmarks, navigation aids, radar marks and distances.
Sharing the vessel's passage plan and pilot's passage plan during the master-pilot exchange enables pilots and bridge officers to identify and account for variables and discrepancies that may affect the safe navigation of the vessel. It also allows the pilot and all bridge team members to reach a common understanding of how the voyage will progress. This “shared mental model,” which includes details such as where and when turns will be made,Footnote 20 is especially important when a pilot's passage plan is not documented. In such cases, the ongoing exchange of navigational information helps the pilot and bridge team work cooperatively to monitor the vessel's position and movement.
The STCW Code emphasizes the importance of an ongoing exchange of information between master and pilot and states that “despite the duties and obligations of pilots, their presence on board does not relieve the master or officer in charge of the navigational watch from their duties and obligations for the safety of the ship.”Footnote 21 Furthermore, in 1995, the Transportation Safety Board (TSB) issued a report in which the Board noted that a pilot's decision making “can become the weak link in a system prone to single-point failure; i.e., in the absence of effective monitoring, there is little safety backup for the pilot in the navigation of the vessel.”Footnote 22 As such, it is important that the bridge team and pilot work cooperatively and share information to avoid a situation where a single-point failure is possible.
The pilot on the Tundra did not have a documented pilotage plan for the occurrence trip, nor is it a common practice for pilots on the St. Lawrence River to have one. Furthermore, the pilot had not obtained an update on the mooring of winter buoys and lifting of summer buoys for his sector prior to any of the pilotage assignments carried out in the previous 3 days.
On the Tundra's passage plan, some waypoints had been marked where the pre-printed course lines on the nautical chart intersected; other waypoints were in reference to the nearest buoy. The vessel's passage plan did not take into account wheel-over positionsFootnote 23 and did not indicate intermediate courses.
Pilot proficiency
The LPA is a federal Crown corporation responsible for providing safe and efficient pilotage services within the St. Lawrence River area. The LPA's major responsibilities include establishing compulsory pilotage areas and issuing pilot licences and pilotage certificates. The LPA contracts 2 corporations of pilots that total 185 licensed pilots and apprentice pilots for operations within 2 districts. The CPSLC covers district No. 1, the sector between Montréal and Québec City, and is divided into 2 zones: Montréal/Trois-Rivières, and Trois-Rivières/Québec City. The Corporation of Lower St. Lawrence Pilots covers district No. 2, the area between Québec City and Les Escoumins.
The LPA contracts the training of pilots to the CPSLC, but retains the responsibility for ensuring pilots are duly trained and licensed. Pilots receive the majority of their training during a 2-year apprenticeship. Upon successful completion of this apprenticeship, a pilot obtains a Class C licence and is limited to working on vessels of a specified maximum length.Footnote 24 After obtaining 2 years of experience in this licence class, the pilot becomes eligible for a licence upgrade. The CPSLC requires pilots to complete 2 days of simulator training before recommending them to the LPA for a licence upgrade. Further licence upgrades require similar combinations of experience and simulator training.
The training that pilots receive during their apprenticeship provides them with local and technical knowledge necessary to safely operate and handle vessels in their pilotage sector. Apprentices learn to use standard navigational practices for passage planning and position fixing, use bridge equipment and other aids to navigation effectively, and make optimal use of all human resources. In addition, pilots obtain knowledge on specific courses and pilotage marks, such as transits, bearings (visual and radar), and distances (visual and radar) taken from fixed objects. During a voyage, these marks are used to both initiate course alterations and continually monitor the vessel's position. Once this local and technical knowledge is imparted to the pilot, it remains their responsibility to maintain sound navigational practices for each pilotage assignment.
Assessment of pilot proficiency
In 1999, the Canadian Transportation Agency (CTA) issued a Review of Pilotage Issues report to the Minister of Transport identifying concerns about a lack of pilot assessments. The report recommended that “the pilotage authorities be required to develop and implement a fair and reasonable system for assessing pilots' competency and quality of service, after consultation with interested parties. This assessment process should take place regularly and not less than every five years.”Footnote 25
In 2008, the Canadian Marine Pilot's Association and the 4 pilotage authorities in Canada,Footnote 26 including the LPA, developed a set of guiding principlesFootnote 27 to help the authorities implement programs to assess pilot proficiency. The guiding principles were intended to allow authorities to meet Recommendation No. 9 of the CTA's Review of Pilotage Issues and IMO Resolution A.960.Footnote 28
There are 9 guiding principles in total, 4 of which are listed below and suggest that pilot assessments be
- applicable to all pilots,
- conducted regularly (not less than once every 3 years),
- conducted using multiple means of assessment,
- focused on offering specific and practical steps to remedy situations should a pilot's proficiency and/or performance need to be improved.Footnote 29
In 2009, the LPA commissioned a reportFootnote 30 that examined methods for competency assessment in 6 pilotage organizations,including 2 in Australia, 3 in the United Kingdom (UK), and 1 in the Netherlands. The report identified that both Australia and the UK have guidelines in place to regularly assess pilot competency: the UK's Port Marine Safety Code requires that pilots revalidate their authorizations every 5 years, with the revalidation process including a competency assessment and the Guidelines for Marine Pilotage Standards in Australia require ongoing competency assessments using check pilots and marine simulators. The report recommended a series of steps for the LPA to undertake in order to develop an ongoing pilot competency assessment program that would involve a combination of simulator-based assessments and check rides. The LPA does not currently have a pilot competency assessment program, whereas the other 3 pilotage authorities have implemented a program. The LPA relies primarily on the report of an accident/incident or a complaint from a vessel owner in order to be apprised of a pilot's conduct.
Use of personal communication devices
In recent years, the use of personal communication devices has been linked to numerous accidents across transportation modes worldwide. The TSB has previously identified the risk associated with the use of cell phones,Footnote 31 and a National Transportation Safety Board reportFootnote 32 on a marine collision determined that distraction and inattentiveness resulting from repeated personal use of a cell phone and laptop computer by the OOW was a probable cause.
In Canada, each province has legislation prohibiting the use of personal communication devices by motor vehicle operators. Furthermore, the rail mode in Canada restricts the use of communication devices to matters pertaining to railway operations, and cellular telephones are not to be used when normal railway radio communications are available.Footnote 33 There are presently no Canadian regulations with respect to the use of personal communication devices in the marine mode. In lieu of specific regulations, the CPSLC Code of Ethics Rule Book and Benefits for Pilots requires that “When piloting a vessel, the pilot must apply their full attention to the task of piloting. Any irrelevant activity that can distract from the piloting task is incompatible with this obligation.”Footnote 34
As the Tundra was proceeding downriver, the pilot used his cellular phone for 5 personal calls lasting a total of approximately 46 minutes. One individual call lasted for 30 minutes. In addition, 6 personal text messages were sent/received. The pilot was not using his cell phone at the time of the missed course change or at the time of the grounding. There had been no mobile communications in the 59 minutes prior to the grounding.
Fitness for duty
The General Pilotage Regulations require every licensed pilot to undergo a medical examination at least once every 2 years.Footnote 35 The examinations, conducted by LPA-designated physicians, are used to determine whether pilots are medically fit to carry out their duties effectively. As part of the examination, pilots are to be assessed for “a disorder that could prevent the applicant or holder from reacting effectively while performing pilotage duties.”Footnote 36 The regulations also contain a requirement for pilots to report to their pilotage authority if they are no longer physically or mentally fit to perform duties. The LPA may, at any time, request that a medical exam be performed if it has reason to believe that the licence holder's health presents a risk to safety.
Fatigue
Sleep is a fundamental biological need that must be satisfied. If it is not, a sleep debt can result, either because of the significant reduction of a single sleep period (acute sleep loss) or because of a sleep debt that is built up over time (accumulated sleep loss).
A pilot's work may involve irregular and lengthy work hours, night shifts, unpredictable duty rosters, and commutes of various distances to and from their assignments. These factors can significantly contribute to fatigue among pilots by affecting how much restorative sleep they obtain. Non-work-related factors (i.e. personal issues, aging, medical problems, and alcohol use) can also limit a pilot's opportunity to obtain restorative sleep. The IMO recognizes that certain medical conditions increase fatigue and impair work performance, in particular sleep disorders such as obstructive sleep apnea and insomnia.Footnote 37
Performance decrements associated with fatigue can include, for example, slowed (or no) reaction time, reduced vigilance, impaired decision-making, inability to concentrate, poor judgment, poor memory, distraction, and loss of awareness in critical situations.Footnote 38 In extreme cases, excessive fatigue can lead to micro-sleeps, which are uncontrollable sleep periods of short duration (between a few seconds and a couple of minutes), when a person is often unaware. Micro-sleep lapses have been well-documented internationally as causal factors in a number of maritime, and other, transportation incidents.Footnote 39
Circadian rhythm sleep disorders
Circadian rhythm sleep disorders involve difficulty initiating and maintaining sleep; in addition, sleep that is experienced is non-restorative or of poor quality. A particular type of circadian rhythm sleep disorder, known as shift work disorder,Footnote 40 may occur when there are frequent changes in an individual's shift work schedule and when the work hours overlap with the individual's normal sleep period.Footnote 41 Persons with co-existing medical, psychiatric, and sleep disorders, such as obstructive sleep apnea, and individuals with a strong need for stable hours of sleep may be at particular risk for this disorder.
Obstructive sleep apnea
Obstructive sleep apnea is a medical disorder caused by partial or complete obstruction of airflow through the pharynx during sleep. This obstruction of airflow disrupts and fragments sleep and, consequently, can impair one's performance during wakefulness. Individuals with obstructive sleep apnea may be unaware of the frequent arousals and awakenings that they experience during sleep.Footnote 42 In fact, it is common for individuals with obstructive sleep apnea to report that they sleep very well. This is because their fragmented sleep produces excessive sleepiness which in turn allows them to fall asleep quickly and resume sleep within seconds of awakening.
The prevalence of obstructive sleep apnea in the general public has been estimated to be 4% in men and 2% in women.Footnote 43 Some estimates indicate a higher prevalence (as high as 10%) for men between the ages of 40 and 60,Footnote 44 especially if they are overweight. Obstructive sleep apnea is more common in people who snore,Footnote 45 and is reliably linked to obesity.Footnote 46 In addition, smoking or allergies can potentially exacerbate sleep-disordered breathing by causing inflammation of the upper airway tissues. Alcohol use in people with untreated obstructive sleep apnea also aggravates sleep-disordered breathing.Footnote 47
The pilot on the Tundra was involved in a similar accident in 2004, when the container vessel Horizon grounded at the same location as in this occurrence. In the TSB reportFootnote 48 that followed, one of the findings as to cause stated that fatigue may have been a factor in the pilot's decreased vigilance at a critical time. As a result of the Horizon grounding, the pilot underwent a sleep evaluation in 2007 at the LPA's request; however, he did not receive any feedback regarding the outcome of that evaluation, nor did the LPA due to patient–physician confidentiality. The diagnosis from the sleep evaluation was that the pilot's sleep was “fragmented by numerous returns to wakefulness, probably compatible with shift worker insomnia.” He was not diagnosed with obstructive sleep apnea at that time. The pilot remained in service and subsequent biennial medical examinations required to determine fitness for duty made no mention of a sleep disorder.
At the time of the Tundra's grounding, the pilot had the following risk factors commonly found in obstructive sleep apnea sufferers: elevated body-mass index, use of cigarettes, environmental allergies, asthma, snoring, and previous difficulties with sleep, as well as the demographic risk factor of being middle-aged. The pilot was requested by the TSB to undergo a sleep evaluation, which he did on 30 April 2013. This sleep evaluation included a comprehensive examination of physical features that can contribute to sleep-disordered breathing. As a result of the 2013 sleep evaluation, the pilot was diagnosed with mild, positional, rapid eye movement-related obstructive sleep apnea and shift work disorder.
Pilot's hours of work and rest
In the 3 days prior to the occurrence, the pilot's hours of work and rest were as follows:
- On 25 November, he awoke at 0600 to work an unscheduled job between 0800 and 1530 and retired for bed at around midnight.
- On 26 November, he awoke at approximately 0900 and spent the day in Montréal taking care of work-related matters. He went to sleep at approximately 2330.
- On 27 November, he awoke at 0800 and worked a shift from 1500 to 2200. He went to sleep at approximately 0100 on 28 November.
- On 28 November, he awoke at approximately 0800 and remained awake until starting his work shift aboard the Tundra at approximately 1830. The incident took place at 2148 that evening, at which point the pilot had been awake for approximately 14 consecutive hours.
Fatigue awareness for pilots
In 2002, Transport Canada (TC) developed a fatigue management program for marine pilots. The program was developed in response to the CTA Review of Pilotage Issues of 1999 and the following TSB recommendation:
The Department of Transport and the Canadian Pilotage Authorities develop and implement an awareness program to provide guidance to operational employees, including pilots on reducing the adverse effect of fatigue on job performance.
Transportation Safety Recommendation M99-04
Canadian pilotage authorities responded positively, and fatigue awareness programs were initiated. Non-mandatory fatigue information sessions were made available to LPA pilots beginning in 2003, and continued to be available on a voluntary basis through 2004.
In subsequent years, fatigue awareness was incorporated as part of the CPSLC's apprentice pilot training program. The pilot attended a session on fatigue management in the year 2000 as part of a BRM training course. He had not participated in any fatigue-related training since then.
The issue of pilot fatigue has been raised in previous Board reports. Following the grounding of the Horizon in 2004, the Board issued a safety concern stating that “despite fatigue awareness training and contractual arrangements that set out adequate rest for pilots, fatigue continues to be a factor in occurrences.”Footnote 49
Alcohol use
The LPA has a policy on drug and alcohol useFootnote 50 that covers drug and alcohol testing, allowable blood-alcohol content while on duty,Footnote 51 medication use, use of illicit drugs, and issues relating to employees' treatment for addiction issues. According to the policy, the LPA can order a drug or alcohol test when it has reason to believe that a pilot (or any other LPA employee occupying a safety-sensitive position) is under the influence of drugs or alcohol.
The LPA Regulations preclude applicants from being awarded a pilotage licence or certificate if they have been convicted of a criminal offence under section 253 of the Criminal Code.Footnote 52 However, the regulations do not require the suspension or revocation of the licence of a pilot who is convicted of the same offences once he or she has been licensed for more than 1 year.Footnote 53 Further, the LPA has no requirement or procedure for pilots to report such convictions.
Within the United States, marine pilots are subject to both federal and state regulations. Under federal regulations, which are administered by the United States Coast Guard (USCG), a pilot who is in possession of a valid licence is not required to report a driving under the influence (DUI) conviction to the USCG, but a pilot applying for or renewing a pilot's licence is required to report such a conviction. The USCG, however, may suspend or revoke a valid licence because of a DUI conviction at any time. Under some state regulations (e.g. New Jersey), pilots who hold valid licences are obligated to report a DUI conviction to the state, as are pilots renewing or applying for licences.
In contrast, in the US aviation industry, pilots are required to report DUI arrests, administrative actions, and convictions.Footnote 54 When such an offence is reported, a preliminary investigation is initiated to ensure that there are no other reportable actions. Subsequent investigation can result in denial or suspension of a pilot's medical certificate for a period of up to 1 year. Research has found that general aviation pilotsFootnote 55 who have a history of DUI convictions are up to 43% more likely to have an aviation accidentFootnote 56 compared to pilots who do not have a history for the following reasons:
- pilots with a DUI history are more likely than other pilots to fly after drinking;Footnote 57
- DUIs may be an indicator of chronic drinking problems that can affect cognitive functions and health, which in turn may compromise pilot performance; and,
- pilots with a DUI history are at an increased risk of crash involvement because they are more prone than other pilots to risk-taking in general.Footnote 58
Because of the increased accident risk for pilots with a DUI history, background checking for DUI history may reduce both alcohol-related and non-alcohol-related crashes.
In 2008, the pilot received 2 separate 30-day administrative licence suspensions that led to 2 DUI convictions under the Criminal Code.Footnote 59 These convictions and licence suspensions were not reported to the LPA or the CPSLC, nor were they required to be reported under current legislation.
Previous occurrences and recommendations
The TSB has previously identified the need for pilots and bridge teams to exchange information on passage plans and work collaboratively to monitor the vessel's progress. TSB Investigation Report MS9501 (A Safety Study of the Operational Relationship between Ship Masters / Watchkeeping Officers and Marine Pilots), found that monitoring of vessel movements is critical to safe navigation in compulsory pilotage waters and is dependent on effective communication among the bridge team. In order to effectively monitor the vessel movements and assist the pilot in maintaining situational awareness, it is necessary that the master and OOW know the pilot's passage plan and provide the pilot with feedback on the vessel's position relative to the plan.
The Board has previously recommended that:
The Department of Transport require that the pilotage authorities publish official passage plans for compulsory pilotage waters and make them available to masters to facilitate monitoring of the pilot's actions by the vessel's bridge team.
Transportation Safety Recommendation M94-34
Although TC did not accept this recommendation, the Board notes that inadequate monitoring of a vessel's position is frequently associated with groundings and strikings. The Board considers close and continuous monitoring of a vessel's progress using a shared passage plan to be essential for the safe conduct of the vessel. Accordingly, the Board further recommended that:
The Department of Transport require that pilots, as part of their initial hand-over briefing:
- obtain the master's agreement to the intended passage plan; and,
- invite the bridge team's support by having the officer of the watch plot and monitor the vessel's position at regular intervals and report the position to the pilot with respect to the agreed passage plan.
The grounding of the Federal Agno (M09C0051) and striking of the Petersfield (M09W0193) further exemplify that the issues of agreeing on a common passage plan and continuously monitoring a vessel's position remain relevant in the compulsory pilotage waters of Canada.
Subsequent to the investigation into the striking of the Common Spirit (M12L0095), the Board identified the lack of pilot proficiency assessments to be a finding as to risk and issued a safety concern stating the following:
The Board is concerned that, without standardized and documented assessments of on-board performance, there is a risk that apprentices without the necessary skills and expertise may be issued pilot licences. Furthermore, if periodic, standardized, and documented proficiency assessments are not carried out, the Board is concerned that licensed pilots may not maintain the skills and expertise necessary for safe pilotage.
The LPA has indicated that periodic evaluation of pilot proficiency will take place and is aiming to fully implement a program in this regard by July 2014. The LPA is also currently working on the creation of a training committee composed of the LPA, the CPSLC, and the Corporation of Lower St. Lawrence Pilots that will evaluate the competency of apprentice pilots.
Analysis
Events leading to the grounding
In this occurrence, the pilot did not use all available resources to safely navigate the vessel. Prior to departure, he had not made himself aware of the status of buoys within his pilotage zone, despite the fact that he was primarily using them to pilot the vessel. In addition, the pilot's passage plan contained intermediate courses that were not marked on the vessel's passage plan, but the vessel's passage plan was not verified by the pilot and therefore the discrepancies went unidentified. As the vessel proceeded downriver, there was little communication between the pilot and the other members of the bridge team, who were not informed as to the pilot's intentions prior to course changes.
As the vessel neared a planned intermediate course change, the pilot was seated on the port side of the bridge at a distance of approximately 8 m from the rest of the bridge team and in a position where the next set of range lights would not be visible. The pilot had planned to initiate this intermediate course change when buoy S-140 was abaft of the vessel; however, the buoy had been removed 7 days earlier, and the turn was not initiated. The next lateral buoy visible on the vessel's port side was the S-136, but its light characteristics differed from those of S-140. As such, it is unlikely that the pilot missed the course change because he had confused these 2 buoys. Rather, it is more likely that the pilot's ineffective monitoring of the vessel's position at this time was due to diminished situational awareness resulting from fatigue. Given that the monitoring by the officer of the watch (OOW) was also ineffective, the vessel continued on its course, exited the channel, and ran aground.
Bridge resource management
Three key elements of bridge resource management (BRM) are monitoring the vessel's progress, sharing the passage plan, and maintaining situational awareness. In this occurrence, the vessel's passage plan and the pilot's passage plan differed, but the master and pilot had not discussed the plans and therefore the pilot and the bridge team were unaware that some of their course alteration points differed. Additionally, the lack of communication between the bridge team and pilot while underway, specifically with regard to where course changes were to occur, prevented the bridge team from serving as an effective back-up for the pilot. Language and cultural differences may have contributed to challenges in bridge team communication. Because eastern European cultures tend to be higher on the power distance dimension than western cultures like Canada,Footnote 60 the Ukrainian crew members may have been less likely than individuals from other, western cultures to question the pilot's authority regarding the course of the vessel. Furthermore, the pilot's physical position on the bridge in relation to the other crew members was not conducive to the initiation and/or maintenance of effective communication among bridge team members.
Although marine pilots and marine pilot applicants within Canada are required to complete BRM training, this training alone may not be sufficient to ensure that BRM is being effectively implemented on board vessels. As demonstrated in this occurrence, in spite of previous BRM training, the pilot did not use effective BRM techniques, suggesting that training transferFootnote 61 had not occurred. Effective training transfer can be accomplished by having employees perform certain activities to more effectively and quickly apply skills they have learned during training. For example, providing opportunities to practice a new skill increases the likelihood of training transfer, as does follow-up with trainees and supervisors regarding goals and action plans. Linking training with performance management and development processes can further help foster accountability for follow-up and learning among trainees.Footnote 62,Footnote 63 With respect to marine pilots, further guidance on BRM implementation and regular pilot assessments may help to ensure that BRM training is successfully implemented on board.
If bridge team members do not share a complete and common understanding of a vessel's intended route and continuously exchange information, there is a risk that the bridge team members' ability to monitor a vessel's progress may be compromised.
Proficiency assessments for pilots
It is common practice in most workplaces for employees to undergo regular performance assessments to ensure they continue to possess the knowledge and skills required to effectively perform their duties. In this occurrence there were several examples that demonstrated the pilot was not exercising best practices for pilotage:
- relevant Notices to Shipping for the pilotage zone, specifically those with regards to the buoy program status, were not consulted;
- the vessel's passage plan was not verified to determine if it matched the pilot's passage plan;
- the vessel's progress was monitored primarily using buoys and was not cross-referenced by other means;
- the information exchanged between the pilot and other members of the bridge team was minimal; and,
- the pilot used a personal communication device as he was piloting the vessel.
Pilots under the Laurentian Pilotage Authority (LPA) are not required to undergo any formal proficiency assessments once they have been issued a license. In contrast, the 3 other Canadian pilotage authorities have established procedures for ensuring the continued proficiency of their pilots. The primary method that the LPA currently uses to check a pilot's record is a database of reported accidents, incidents, and complaints.
A proficiency assessment of the pilot in this occurrence may have identified practices that were incompatible with his obligation to safely conduct the navigation of the vessel. Proficiency assessments may also be a first step in providing pilots with necessary feedback while also raising the LPA's awareness about issues regarding pilot proficiency.
If regular pilot proficiency assessments are not conducted, there is a risk that unsafe pilotage practices may continue unchecked.
Pilot's fitness for duty
It is imperative that individuals who occupy safety-critical positions are fit for duty and therefore able to perform the full range of tasks that may be expected of them. To this end, the General Pilotage Regulations require marine pilots to undergo examinations at least once every 2 years. However, these examinations are largely dependent on self-reporting by the patient and lack the scope to detect some types of disorders (such as sleep-related disorders) that may impact a pilot's performance.
Although the pilot in this occurrence had undergone a sleep evaluation in 2007 following the Horizon occurrence, neither he nor the LPA received any feedback on the outcome of that evaluation, and so were likely unaware of the ongoing risk posed by his lifestyle factors and fatigue. The pilot had also undergone subsequent periodic medical examinations as required by the regulations, but they did not reveal the existence of any sleep disorders or a requirement for further testing.
The importance of fatigue awareness training programs is underscored by the fact that individuals with sleep disorders are often unaware of the disorder and may not recognize the symptoms in themselves. In these cases, awareness training can help pilots identify the adverse effects of fatigue and, if necessary, seek help to manage sleep-related disorders.
The LPA offered voluntary fatigue awareness training to all pilots from 2003 to 2004, at which time this training was stopped. The pilot apprenticeship program now contains a module on fatigue. While offering fatigue awareness training is a positive step in helping pilots identify and manage the adverse effects of fatigue, it is important that this training be available to all pilots on a regular basis, and not just once during a pilot's apprenticeship years.
If pilots are not trained in fatigue awareness, there is a risk that they may not be able to identify the symptoms or signs related to sleep disorders that are not detectable through a regular medical exam.
Fatigue
Although an analysis of the pilot's 72-hour sleep history indicated that he was not suffering from a significant acute or chronic sleep debt at the time of the occurrence, there were other risk factors and indicators of fatigue. The pilot's untreated obstructive sleep apnea and shift worker disorder likely reduced the quantity and quality of his sleep on the nights leading up to the occurrence, increasing his risk for fatigue. The physical environment of the bridge, which was dark and warm with the presence of monotonous engine noise, and the time of day (evening), would have been conducive to sleep, especially for individuals with sleep disorders. As well, his physical location on the bridge reduced his interaction with other crew members and, in the 10 minutes preceding the grounding, the relatively abrupt cessation in his level of activity suggests that the pilot may have experienced a micro-sleep.
Driving under the influence reporting requirements
Driving under the influence (DUI) convictions can be indicative of alcohol use problems. Formal requirements for employees in safety-critical positions to report such convictions may assist employers in identifying and managing such problems. While the US aviation industry has recognized the significance of DUI convictions for air pilots and some states have requirements for marine pilots to report DUI convictions, neither the Canadian aviation industry nor the Canadian marine pilotage authorities have similar reporting requirements. The pilot had 2 previous DUI convictions and licence suspensions that had not been reported to the LPA, the Corporation des Pilotes du Saint-Laurent Central (CPSLC), or Transport Canada, nor were they required to be under current legislation.
Alcohol use was not found to be a factor in this occurrence. However, if Canadian pilotage authorities do not have a DUI reporting policy for licenced/certificated pilots, those experiencing alcohol-related problems that affect performance may not be identified and treated, increasing the risk of accidents.
Situational awareness and personal communication devices
The use of personal communication devices (such as cellular telephones) may diminish situational awareness, a fact that is especially concerning when attention to safety-critical tasks is required. Some modes of transportation have recognized this risk and have enacted legislation limiting or prohibiting the use of such devices.
The CLSPC does not have a specific rule or protocol regarding the use of personal communication devices; however, they do advise that pilots apply their full attention to the task of piloting, as any irrelevant activity can distract from the task. In this occurrence, the pilot used his personal communication device for several personal phone calls and text messages as the vessel was underway. While these communications were not causal to the accident, they did occur at a time when the pilot was engaged in the conduct of the vessel, limiting his ability to focus on its safe pilotage.
If pilotage organizations do not institute specific rules or protocols to govern the use of personal communication devices while piloting, pilots may not understand the associated risks and may continue to use them at any time while piloting.
Findings
Findings as to causes and contributing factors
- The pilot's passage plan was not documented or communicated to the bridge team, nor was the vessel's passage plan verified by the pilot.
- The pilot and other members of the bridge team were not exchanging information pertaining to the navigation of the vessel; as such, the bridge team was unaware of a planned course change.
- The pilot did not use all available navigational resources in piloting the vessel.
- The pilot did not carry out a planned course change and, as a result, the vessel exited the channel and ran aground.
- Fatigue was a likely factor in the pilot's diminished situational awareness at a critical time when a course change was required.
Findings as to risk
- If bridge team members do not share a complete and common understanding of a vessel's intended route and continuously exchange information, there is a risk that the bridge team members' ability to monitor a vessel's progress may be compromised.
- If regular pilot proficiency assessments are not conducted, there is a risk that unsafe pilotage practices may continue unchecked.
- If pilots are not trained in fatigue awareness, there is a risk that they may not be able to identify symptoms or signs related to sleep disorders that are not detectable through a regular medical exam.
- If Canadian pilotage authorities do not have a driving under the influence (DUI) reporting policy for licenced/certificated pilots, those experiencing alcohol-related problems that affect performance may not be identified and treated, increasing the risk of accidents.
- If pilotage organizations do not institute specific rules or protocols to govern the use of personal communication devices while piloting, pilots may not understand the associated risks and may continue to use them at any time while piloting.
Safety action
Safety action taken
Owner
The owner sent a message addressed to the entire fleet to remind officers of the watch to regularly verify/monitor the vessel's course when the vessel is under the conduct of a pilot. This issue is to be discussed at the next safety meeting and feedback will be communicated to the company.
Laurentian Pilotage Authority
In regards to fatigue awareness training, the Laurentian Pilotage Authority (LPA) and the Corporation des Pilotes du Saint Laurent Central (CPSLC) reached an agreement to undertake a study on the risks related to fatigue.
In addition, the LPA, in collaboration with the CPSLC and the Corporation of Lower St. Lawrence Pilots, published a brochure on the master-pilot exchange. This brochure is provided by the pilot to the master upon boarding. The brochure details particulars of the exchange and covers topics such as the steering system, anchors, radio communication, and manoeuvring.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .
Appendices